

Impact of COVID-19 disease on the male factor in reproductive medicine – how-to advise couples undergoing IVF/ICSI
Julia Stark A * , Stefan P. Kuster B and Vera Hungerbühler C
A * , Stefan P. Kuster B and Vera Hungerbühler C
A
B
C
Abstract
The COVID-19 pandemic has caused widespread concern about its potential impact on various aspects of human health.
This narrative review aims to summarise the current knowledge about the impact of COVID-19 on sperm quality and its effect on assisted reproductive technology.
In this narrative review, a literature search using the PubMed and MEDLINE databases was conducted to identify relevant original research articles published up to 29 January 2023.
Thirty original studies were included in our review. There is evidence that SARS-CoV-2 is detectable in seminal fluid during the acute phase of infection and for up to 1 month. However, the fact that SARS-CoV-2 is barely detectable in semen makes sexual transmission very unlikely. COVID-19 infection has been associated with the following changes in sperm quality: morphology, altered motility, changed DNA fragmentation-index (DFI), decreased sperm concentration, lower total number of sperm, and a significant increase in leukocytes and cytokines. The effects mostly seem to be reversible and have not been shown to negatively affect the outcome of assisted reproductive technology but should lead to further research concerning the health of the offspring, because a correlation of increased DFI after COVID-19 even 5 months after disease could be assumed.
The findings of this narrative review suggest that SARS-CoV-2 may harm sperm quality in the acute phase.
A recovery time of at least 3 months regarding assisted reproductive therapy could be reasonable.
Keywords: COVID-19, infertility, insemination, male factor, male hormones, reproductive medicine, SARS-CoV-2, sperm quality, semen parameters.
Introduction
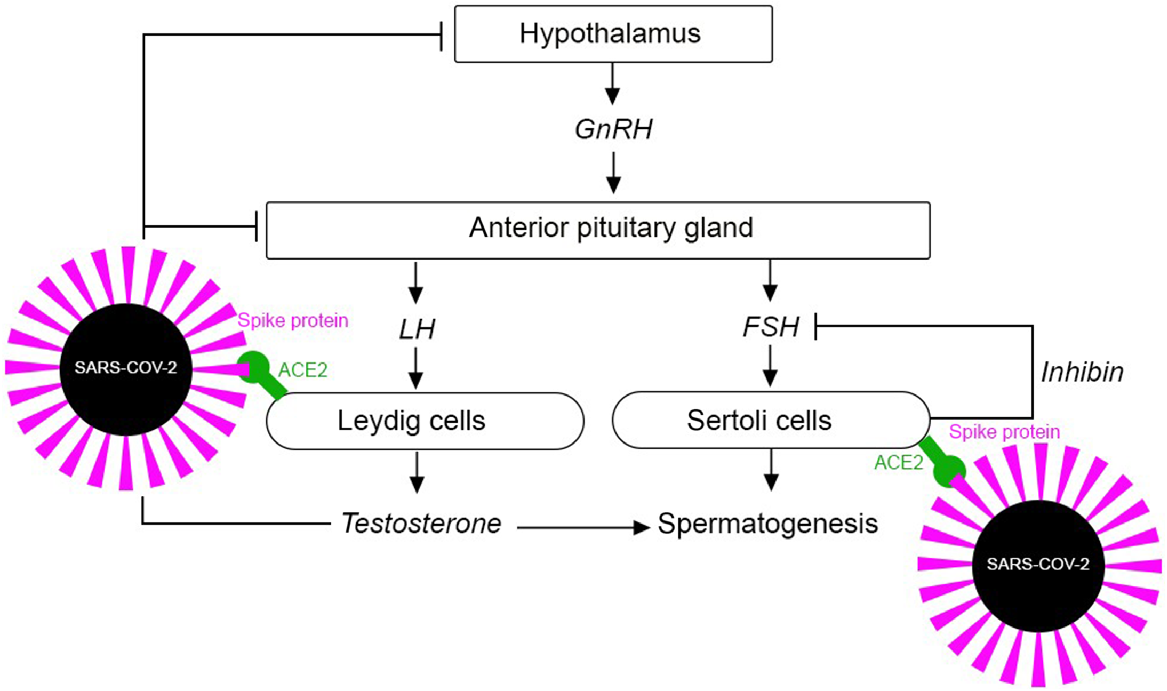
Coronavirus disease 2019 (COVID-19) was declared a pandemic by the World Health Organization on 11 March 2020 (Chauhan 2020). The clinical appearance of infections with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) can vary from asymptomatic infection to severe illness and death (Kakodkar et al. 2020). SARS-CoV-2 enters target cells through interaction between the cellular ACE2 receptor and the virus spike proteins (Moshrefi et al. 2021). ACE2 is found not only in the respiratory system, but also in the male reproductive system, where ACE2 is expressed in spermatogonia, Sertoli cells and Leydig cells (Wang et al. 2020) (Fig. 1). Speculation about sexual transmission of SARS-CoV-2 and its impact on fertility has therefore appeared in medical literature since the beginning of the COVID-19 pandemic, and medical professionals have been approached regularly by couples experiencing idiopathic infertility over the past few years, seeking answers to their questions about the impact of SARS-CoV-2 on reproductive health. Focusing on the impact of SARS-CoV-2 on male fertility seems of paramount importance. The discussions increased further once COVID-19 vaccines became available, triggering even more questions and speculation about potential adverse effects on fertility.
In the fast-evolving field of COVID-19, it has become difficult to keep track of the most recent scientific developments. In addition, as already mentioned by Ata et al. (2023), there are still many open questions concerning the male factor, such as the impact of prior SARS-CoV-2 infection of the male partner on therapy outcomes in reproductive medicine, or defining a minimum interval between COVID-19 and infertility therapy. Thus, to support other medical professionals in providing evidence-based advice for their patients for daily counselling on idiopathic infertility, we aimed to answer the following questions in a narrative review, with a focus on the male factor: (1) Is SARS-CoV-2 sexually transmitted? (2) Is sperm quality reduced – and if so, how long – after SARS-CoV-2 infection? and (3) Does COVID-19 disease have any effects on the outcome of assisted reproductive technology (ART)?
To find well-founded answers to these questions, we have compiled what could be useful for everyday counselling to be able to advise couples experiencing idiopathic infertility. In this narrative review, we focus on the male factor because it is rarely discussed, but very important, especially for couples undergoing in vitro fertilisation/intracytoplasmic sperm injection (IVF/ICSI).
Methods
Our population of interest was men of reproductive age with COVID-19 disease. The outcome of interest was the effect of COVID-19 disease on the male factor in reproductive medicine (semen quality and outcomes of IVF/ICSI in couples). We did not include studies that focused on the impact of COVID-19 vaccines, because this will be discussed in another paper.
Search strategy
The relevant studies were searched from the electronic databases PubMed and MEDLINE, using the following keywords: ‘COVID sperm’, ‘SARS-CoV-2 sperm’, ‘COVID-19 sperm fertility’, ‘COVID insemination’, ‘SARS-CoV-2 IVF’, ‘sperm quality’. The search was last performed on 29 January 2023. Furthermore, the reference lists of the included studies were manually searched to find additional studies.
Eligibility criteria
Only studies with primary data were used. Case reports, case series, and reviews (systematic or narrative) were excluded. We also excluded studies focusing on females. Study selection/data extraction: two researchers (JS, VH) were involved in the data synthesis process. To process the data, we used Zotero (version 6.0.21, available at https://www.zotero.org/download/) to collect, organise, and cite research.
Results
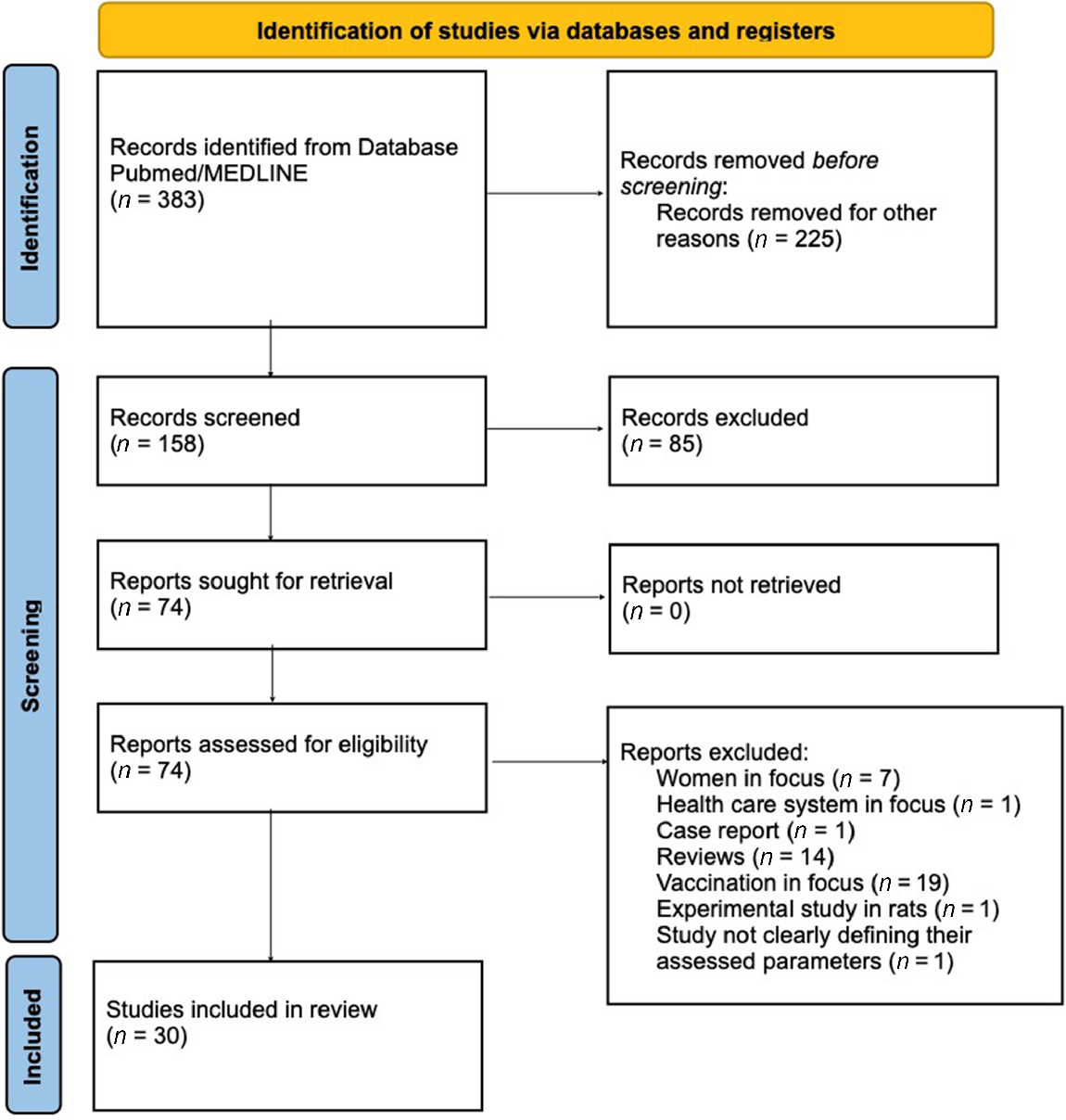
Our search identified 383 articles (Fig. 2). After title and abstract screening, 74 articles underwent full-text screening. Forty-four articles were excluded due to the following reasons: women in focus (n = 7), healthcare system in focus (n = 1), case report (n = 1), reviews about COVID-19 and fertility (n = 14), vaccination in focus (n = 19), an experimental study in rats (n = 1), and a study not clearly defining their assessed parameters (n = 1). Eventually, 30 studies were included in this review (Table 1).
| Study | Year of publication, city, country | Type of study | Inclusion/exclusion criteria | Study groups (male) | Parameter | |
|---|---|---|---|---|---|---|
| Li et al. (2020a), Clinical characteristics and results of semen tests among men with coronavirus disease 2019 | 2020, Beijing, China | Cohort study | Inclusion: aged 15 years and older. COVID-19 was defined as a positive result for SARS-CoV-2 in real-time reverse transcriptase–polymerase chain reaction assay of nasal and pharyngeal swabs | n = 38 | Using reverse transcriptase–polymerase chain reaction assay to detect SARS-CoV-2 in semen. | |
| Exclusion: inability to provide a semen specimen because of erectile dysfunction, being in a comatose state, or dying before recruitment | ||||||
| Ma et al. (2021), Evaluation of sex-related hormones and semen characteristics in reproductive-aged male COVID-19 patients | 2021, Wuhan, China | Cohort study | Inclusion: reproductive-aged men | Semen of n = 12 men, sex-related hormone levels of n = 119 infected men, n = 273 control men | COVID-19 disease and its effect on male hormonal changes. Detection of SARS-CoV-2 in semen using qRT-PCR. The time between semen collection and disease onset ranged from 56 days to 109 days (with a median of 78.5 days). | |
| Temiz et al. (2021), Investigation of SARS-CoV-2 in semen samples and the effects of COVID-19 on male sexual health by using semen analysis and serum male hormone profile: a cross-sectional, pilot study | 2021, Bagcilar/Istanbul, Turkey | A cross-sectional, pilot study | Inclusion: age 18–60 years, laboratory-confirmed COVID-19 patients immediately after their treatment, highly suspected COVID-19 patients with specific CT imaging findings before treatment | n = 30 | COVID-19 patients before and immediately after a defined 5-day treatment, and controls. Detection of SARS-CoV-2 in semen comparing demographics, semen parameters, and serum hormone levels. | |
| Exclusion: testicular risk factors such as a history of infertility, history of anatomical/surgical/malignant, or infection risk in the past. Patients who could not meet a 2–5 day ejaculatory abstinence period before semen sampling and could not ejaculate semen were also not included in the study | ||||||
| Guo et al. (2021a), Absence of SARS-CoV-2 in semen of COVID-19 patient cohort | 2021, Jinan, China | Cohort study | Inclusion: males aged 20–62 years, median interval from 32 days from diagnosis to providing semen samples. Strict hygienic rules were established to avoid virus contamination before masturbation/ejaculation | n = 23 male patients | COVID-19 disease and influence on total sperm counts, total motile sperm counts, and sperm morphology. Detection of SARS-CoV-2 in semen using RT-qPCR assay. The time interval from diagnosis to semen samples acquired is approximately 32 days (27.5–33 days). | |
| Holtmann et al. (2020), Assessment of SARS-CoV-2 in human semen – a cohort study | 2020, Duesseldorf, Germany | Cohort study | Men with a positive swab result or positive IgA and IgG antibodies were considered to be positive for COVID-19. Patients were classified as having a mild COVID-19 infection when home care was possible. Moderate COVID-19 was defined for patients requiring hospitalisation with up to 6 L oxygen supplied to achieve >92% peripheral oxygenation. The control group consisted of healthy volunteers (no symptoms related to COVID-19 in the previous 8 weeks) with no reported andrological pathology | Recovered men (8–54 days after an absence of symptoms): n = 18, control: n = 14, active COVID-19 infection: n = 2 | COVID-19 disease: analysis of semen quality. Detection of SARS-CoV-2 by RT-PCR in the native semen sample and after density gradient preparation. | |
| Li et al. (2020b), Impaired spermatogenesis in COVID-19 patients | 2020, Wuhan, China | Single-centre, hospital-based observational study (pair of two case-control investigations) | Inclusion: age above 18 years, not receiving any steroidal drug treatment, no history of infertility, no testicular risk factors such as a history of anatomical/surgical or infection/diseases that may influence spermatogenesis | Autopsied testicular and epididymal specimens deceased COVID-19 men n = 6, surgical specimens from male patients other than of COVID-19; recruited recovering COVID-19 inpatients (n = 23), age-matched controls (n = 23) | COVID-19 disease and impairment of spermatogenesis. | |
| Al-Alami et al. (2022), COVID-19 and semen fluid parameters, a retrospective study from infertility clinics | 2022, Amman, Jordan | Retrospective study | (1) Only vaccinated, infected and vaccinated, neither infected nor vaccinated, only infected | (1) n = 354 | Effect on SFA (seminal fluid analysis) parameters by COVID-19 infection/vaccination. | |
| (2) Men before and after infection and/or vaccination | (2) n = 49 | |||||
| Donders et al. (2022), Sperm quality and absence of SARS-CoV-2 RNA in semen after COVID-19 infection: a prospective, observational study and validation of the SpermCOVID test | 2022, Belgium | Prospective observational study | Inclusion: men between the ages of 18–70 years who had suffered a proven COVID-19 infection | n = 118 | Sperm quality and absence of SARS-CoV-2 RNA in semen after COVID-19 infection. Validation of the SpermCOVID test. | |
| Exclusion: refused to provide informed consent, negative test on SARS-CoV-2 RNA PCR and antibodies, vasectomy | ||||||
| Best et al. (2021), Evaluation of SARS-CoV-2 in human semen and effect on total sperm number: a prospective observational study | 2021, Miami, FL, USA | Prospective observational study | Inclusion: men aged 18–70 who had tested positive for SARS-CoV-2 infection | n = 30 | Searching for RNA by RT-PCR in the semen. The affection of total sperm number by COVID-19 infection in recovered men (approximately 37 days (11–64 days) after testing positive for SARS-CoV2 infection). A follow-up was done approximately 90 days later. | |
| Exclusion: prisoners, critically ill, subjects unable to consent, history of mumps, vasectomy, ejaculatory dysfunctions, prior testosterone replacement therapy, history of male factor infertility, history of sexually transmitted infections, unwilling to donate semen | ||||||
| Hamarat et al. (2022), Effect of SARS-CoV-2 infection on semen parameters | 2022, Konya, Turkey | Single-centre study | Inclusion: men aged 22–46 | n = 41 | Recording of semen parameters before (7.74 ± 3.03 month) and after (2.35 ± 1.35 month) SARS-CoV-2 infection. | |
| Exclusion: patients were excluded from the study if they had azoospermia, were under 18 years of age, had undergone assisted reproduction techniques, had any urogenital operations in this period, were using medications that could affect semen parameters, were using steroids for infection treatment | ||||||
| Guo et al. (2021b), Semen parameters in men recovered from COVID-19 | 2021, Hefei, China | Cohort study | Inclusion: men with a median age of 26 (IQR: 22–34), physically normal concerning external genitalia, male secondary sex characteristics, testicular volume, and texture | n = 41 | Sex-hormone-testing and semen samples were assessed at a median time of 76 (IQR: 73–86.5) days after the appearance of symptoms and 56 (IQR: 49–72) days after hospital discharge. Twenty-two of the 41 patients were tested also 84 (IQR: 74–89) days after hospital discharge. The median time between the first and second sampling was 29 (IQR: 28–32.8) days. | |
| Pazir et al. (2021), Impaired semen parameters in patients with confirmed SARS-CoV-2 infection: a prospective cohort study | 2021, Istanbul, Turkey | Prospective cohort study | Inclusion: men aged 18–49 years with semen analyses before COVID-19 within the normal reference range | n = 24 | The median interval between the diagnosis of COVID-19 and obtaining semen samples was 111.5 days. The cohort was divided into two subgroups, those without and with symptoms of fever. | |
| Exclusion: a non-COVID-19 febrile illness in the last three months, previous exposure to empirical treatments, such as anti-estrogens, antioxidants, and gonadotropins; testicular diseases, such as varicocele and undescended testis, which may be associated with deterioration in semen parameters over time; a previous urogenital tract infection history | ||||||
| Delaroche et al. (2021), Evaluation of SARS-CoV-2 in semen, seminal plasma, and spermatozoa pellet of COVID-19 patients in the acute stage of infection | 2021, France | Cohort study | Inclusion: men with mean age 38.8 ± 10.9 years with mean BMI (body mass index) 26.6 ± 4.3 kg/m2 | n = 32 | Assessment of SARS-CoV-2 presence in the semen of COVID-19-positive patients within 24 h of positive COVID-19 test in nasopharyngeal swab (median interval of 4 days from onset of symptoms to semen collection). | |
| Exclusion: if participants refused, did not answer, could not participate because of severe pathologies, failed to provide a semen sample, if the interval from onset of symptoms to semen collection was too long | ||||||
| Ruan et al. (2021), No detection of SARS-CoV-2 from urine, expressed prostatic secretions, and semen in 74 recovered male patients: A perspective and urogenital evaluation | 2020, Wuhan, China | Cohort study | Inclusion: men median aged 31 years (IQR: 27–36; range 21–49) in recovery state (lessened symptoms and two continuous negative SARS-CoV-2 nucleic acid tests) | n = 74 | Expressed prostatic secretions (EPSs), urine, and semen samples were collected for SARS-CoV-2 RNA detection, and semen quality was analysed (sperm concentration, semen volumes, total sperm counts, morphologically normal spermatozoa, motile spermatozoa, DNA fragmentation index (DFI), movement variables). | |
| Exclusion: men with other acute illnesses or severe chronic diseases, history of mumps infection, semen volume less than 1.5 mL | The median interval between the last positive pharyngeal swab RT-PCR test and semen samples collection was 80 days (IQR: 64–93). Also, hormonal profiles were analysed. | |||||
| Burke et al. (2021), A cohort study of men infected with COVID-19 for presence of SARS-CoV-2 virus in their semen | 2021, Orlando, FL, USA | Cohort study | Inclusion: men with a median age of 32 (range, 24–57), asymptomatic to moderate symptomatic, not requiring hospitalisation | n = 18 | They subjected the semen samples to viral RNA extraction and then processed them by real-time RT-PCR to detect the presence of SARS-CoV-2 RNA. | |
| Exclusion: men who had a vasectomy, taking testosterone or hormonal treatment, with an urologic condition that inhibits ejaculation, undergoing chemotherapy, with a concurrent chronic or acute infection, on immunosuppressant medication | The length of time from diagnosis to semen sample was 1–28 days (median, 6 days). To avoid contamination the study participants were instructed to clean their hands and penis as well as avoid saliva during collection. | |||||
| Paoli et al. (2023), Male reproductive health after 3 month from SARS-CoV-2 infection: a multicentric study | 2022, Rome and Latina, Italy | Multicentric study | Inclusion: men aged 18–65 years and a previous nasopharyngeal swab positive for SARS-CoV-2 | n = 80 compared with two age-matched healthy pre-COVID-19 control groups: | Three months after COVID-19 recovery they performed a physical examination, semen analysis (volume, sperm concentration, total sperm number, progressive motility, abnormal forms), anti-sperm antibodies (ASA) testing, testicular ultrasound, sperm DNA integrity evaluation (TUNEL), sex hormone profile (total testosterone, LH, FSH, prolactin (PRL)), erectile function. Around 88% of patients reported the presence of fever during COVID-19 disease. | |
| Exclusion: men with andrological and systemic diseases, genetic syndromes, diabetes, Klinefelter’s syndrome, and other chromosomal conditions, hypogonadism (total testosterone below 8 nmol/L), neoplasms, recent urinary tract infections, previous chemotherapy and/or radiotherapy treatments, clinically relevant varicocele (clinical grade III) or any other andrological condition known to affect semen parameters and sperm DNA integrity | CTR1: normozoospermic subjects | |||||
| CTR2: primary infertile subjects | ||||||
| Hajizadeh Maleki and Tartibian (2021), COVID-19 and male reproductive function: a prospective, longitudinal cohort study | 2021, Teheran, Iran | A prospective longitudinal cohort study | Inclusion: normal outcomes on fertility evaluation as proven by a urology expert, SARS-CoV-2 infected men aged 34.7 ± 6.3 years, healthy controls aged 33.9 ± 7.5 years | COVID-19 patients (n = 84), 1/84 diagnosed mild-type, 23/84 moderate type, 27/84 severe type, 33/84 critical type, healthy controls (n = 105) | Markers of inflammation, and oxidative stress, apoptotic variables, seminal ACE2 activity and semen quality parameters were evaluated at 10-day intervals for a maximum follow-up time of 60 days among male patients with laboratory-confirmed SARS-CoV-2 infection. | |
| Exclusion: preexisting conditions and infertile factors | ||||||
| Dipankar et al. (2022), Semen quality in males suffering from COVID-19: a pilot study | 2022, Patna, India | Pilot study | Inclusion: 19–45 years aged COVID-19-positive, married males having at least one child, with mild symptoms, not suffering from dyspnea, and abstinence period of 2–7 days | n = 30 | Conduction of real-time reverse transcriptase test (RT-PCR) on all the semen samples. After 74 days of the first sampling, a second sampling was done and checked for volume, viscosity, liquefaction time, agglutination, pH, vitality, progressive motility, sperm count, total sperm count, normal morphology, head defect, neck defect, tail defect, cytoplasmic droplet, white blood count, fructose, DFI (DNA fragmentation index). | |
| Exclusion: negative real-time reverse transcription–polymerase chain reaction (RT-PCR) test of SARS-CoV-2 of their nasopharyngeal swab sample, history of infertility, severe COVID-19 disease, history of immunosuppression, sexually transmitted diseases based on the history and earlier investigations, history of alcohol intake, smoking, varicocele, diabetes | ||||||
| Aksak et al. (2022), Investigation of the effect of COVID-19 on sperm count, motility, and morphology | 2022, Adana, Turkey | Cohort study | Inclusion: 20–50 years old men recovered from mild to moderate COVID-19 infection, all of them had hormone levels within limits, non of them were smokers, and had no previous history of varicocele operation or cryptorchidism. The sexual abstinence was between 2–7 days | n = 100 recovered | All of the COVID-19 group males were exposed to COVID-19 infection from 4 months to 1 year ago. Their semen was examined according to the following parameters: volume, concentration, motility, normal morphology, head anomaly, neck anomaly, and tail anomaly. | |
| Exclusion: COVID-19 disease within the last 3 months, semen volume less than 1.5 mL | n = 100 never had COVID-19 | |||||
| Ertaş et al. (2022), Examining changes on testicular structure and sperm analysis of COVID-19 patients | 2022, Van, Turkey | Prospective study | Inclusion: men with mean age 31 ± 5.67 (19–45) years and BMI 28.41 ± 4.68 kg/m2 | n = 103 | Semen analyses (after at least 3 days of sexual abstinence), FSH, LH, serum total testosterone, Inhibin-B levels, anti-mullerian hormone (AMH) (between 8 AM and 11 AM) were collected and recorded. The median time between semen sample collection and a positive nasopharyngeal swab test was 138 (95–162) days in the SARS-CoV-2 infected group. | |
| Exclusion: history of febrile illness other than COVID-19 in the past 3 months, prior exposure to empirical treatments, such as antioxidants, antiestrogens; patients with a previous diagnosis of urogenital system infection (including orchitis) and testicular abnormalities | (n = 53 COVID-19 positive group, n = 50 COVID-19 negative group) | |||||
| Erbay et al. (2021), Short-term effects of COVID-19 on semen parameters: a multicenter study of 69 cases | 2021, Turkey | Multicentre study | Inclusion: men aged 20–45 years, who had recovered from the disease at least 3 months earlier and who had undergone a spermiogram within the last year before the onset of the disease | n = 69 (divided into 2 groups: n = 26 mild symptomatic (30.4 ± 4.8 years) and n = 43 moderate symptomatic (31.06 ± 4.2 years). In addition, the mild symptomatic group was divided into two subgroups according to the presence or absence of fever | As a standard COVID-19 treatment protocol, the patients with COVID-19 were treated with oral hydroxychloroquine or favipiravir tablets for 5 days. Acetaminophen was administered symptomatically if the patients had fever and pain. Each patient was administered enoxaparin sodium subcutaneously at a dose appropriate for the weight for thromboembolism prophylaxis. | |
| Exclusion: patients younger than 20 and older than 45 years, history of hormonal drug use that could affect spermatogenesis, azoospermia or oligozoospermia, a history of pelvic radiotherapy, history of testicular surgery, those that received medical therapy to increase sperm motility and total sperm number, those that had undergone assisted reproduction techniques | Semen parameters were analysed by semen volume, total sperm number, sperm concentration, total motility, progressive motility, and vitality. | |||||
| Hu et al. (2022), Evaluation of mid- and long-term impact of COVID-19 on male fertility through evaluating semen parameters | 2022, Wuhan, China | Cohort study | Inclusion: male COVID-19 recovered patients aged 31.75 ± 5.77 years old, and the control group aged 31.49 ± 3.10 years old | n = 36 (COVID-19 patients, 86% with fever) | Analysis of sperm quality (pH, volume, concentration, progressive motility, total motility), and alterations of total sperm number with recovery time (first follow-up 83 (64–94) days, second follow-up 175 (150–184) days) were performed. | |
| Exclusion: men with a history of mumps infection, other acute illnesses or severe chronic diseases, or semen volume less than 1.5 mL | n = 45 (controls) | |||||
| Shcherbitskaia et al. (2022), Oxidative stress markers and sperm DNA fragmentation in men recovered from COVID-19 | 2022, St Petersburg, Russia | Cohort study | Inclusion: men aged 32–38 years | n = 17 (COVID-19 recovered patients) | The standard semen parameters (rate of spermatozoa with progressive motility, non-progressive motility, and immotile cells, morphology), its level of sperm DNA fragmentation, and its pro- and antioxidant system state were measured. The median period of recovery was 5 (IQR: 4–7) months. | |
| Exclusion: antioxidant and vitamin supplementation, occupational and environmental exposures to potential reproductive toxins, use of drugs such as habitual drugs, BMI > 25, varicocele, azoospermia, prostatitis, cryptorchidism, sexually transmitted disease, chronic illness, and serious systemic disease, genital trauma, testicular torsion, inguinal or genital surgery, urinary tract infection | n = 22 (control group) | |||||
| Scroppo et al. (2021), COVID-19 disease in clinical setting: impact on gonadal function, transmission risk, and sperm quality in young males | 2021, Milan, Italy | Prospective study | Inclusion: males aged 18–50 years had a positive oropharyngeal swab for SARS-CoV-2 | n = 15 (the patients were divided into two groups (mild and moderate)) | Blood samples (LH, FSH, testosterone, procalcitonin, IL-6, CRP) were taken by 8:30 in the morning. Semen parameters were checked by examination of semen volume, sperm concentration, total sperm number, progressive motility, sperm morphology, and leukocytes detected. | |
| Exclusion: history of co-pathologies that could interfere with the gonadal function | ||||||
| Gupta et al. (2021), Detection of SARS-CoV2 virus using the real-time reverse transcriptase chain reaction in semen and seminal plasma from men with active COVID-19 infection – a pilot study | 2021, New Delhi, India | Cross-sectional study | Inclusion: men with a mean age of 32.2 ± 5.6 years | n = 37 | Within 7 days of symptom onset or 5 days of nasopharyngeal rRT-PCR test positivity in asymptomatic men semen analysis was done for motility and sperm counts. | |
| Exclusion: patients with symptom onset of >7 days, need for ventilatory support, active pneumonia, and presence of comorbidities such as immunocompromised status or on immunosuppressants, diabetes mellitus, or with underlying lung disease | ||||||
| Vahidi et al. (2022), Effect of coronavirus disease (COVID-19) on human semen: no evidence of coronavirus in semen of patients | 2022, Yazd, Iran | Cohort study | Inclusion: men in the acute disease stage but not hospitalised, and men in the clinical recovery stage with no history of hospitalisation in their acute phase, with an acute period of at least 1 month to a maximum of 3 months | n = 40 (n = 20 men in the acute stage, n = 20 men in the clinical recovery) | The semen parameters were compared between the two groups and a PCR test of the patients’ semen was done. | |
| Exclusion: patients with testicular infection, testicular damage, and testicular surgery and those above the age of 45 or under 18 | ||||||
| Koç and Keseroğlu (2021), Does COVID-19 worsen the semen parameters? Early results of a tertiary healthcare centre | 2021, Ankara, Turkey | Cohort study | Inclusion: men aged 23–42 years not needed to be hospitalised | n = 21 | The patients were evaluated in terms of semen parameters, FSH, LH, and testosterone before and at the time of diagnosis of COVID-19. | |
| Exclusion: men with azoospermia | ||||||
| Albeitawi et al. (2022), COVID-19 infection and vaccine have no impact on in-vitro fertilisation (IVF) outcome | 2022, Jordan | A multicentre, retrospective study | Inclusion: vaccinations namely Pfizer (BioNTec), Oxford-Astrazeneca, Sinopharm, IVF procotolls: short agonist protocol, long agonist protocol, flexible GnRH antagonist protocol | n = 151 | Clinical pregnancy rate, implantation rate, fertilisation rate, number of oocytes retrieved, number of mature oocytes, and number, and quality of embryos at day 3 were compared. IVF outcomes in a group of 50 patients who underwent IVF cycles after and before the pandemic were also compared. | |
| Four groups: (a) previously infected with SARS-CoV-2 (n = 18) (b) vaccinated (n = 66) (c) previously infected and vaccinated (n = 34) (d) neither infected nor vaccinated (n = 33) | ||||||
| Wang et al. (2022), Investigating the impact of SARS-CoV-2 infection on basic semen parameters and in vitro fertilisation/intracytoplasmic sperm injection outcomes: a retrospective cohort study | 2022, Wuhan, China | Retrospective cohort study | Inclusion: males with positive results from serum SARS-CoV-2 antibodies, a negative result for nucleic acid tests | SARS-CoV-2 negative group | Measures were semen parameters (volume, semen concentration, total no. of sperm per ejaculate, progressive motility, total no. of progressive motility, complete motility, total no. of complete motility, immotile, total no. of immotile, normal forms, total no. of normal forms) and IVF outcomes (normal fertilisation rate, cleavage rate, high-quality embryo rate, Blastocyst formation rate, available blastocyst rate, fresh embryo transfer cycles, no. of embryos transferred, implantation rate, biochemical pregnancy rate, early miscarriage rate). | |
| Exclusion: missing important information, oocyte donation cycles, total or partial oocyte freezing cycles, lost to follow-up, females with a history of SARS-CoV-2 infection | n = 148 | |||||
| SARS-CoV-2 positive group | ||||||
| n = 50 (n = 26 had undergone one previous semen analysis before infection) | ||||||
| Gacci et al. (2021), Semen impairment and occurrence of SARS-CoV-2 virus in semen after recovery from COVID-19 | 2021, Florence, Italy | Prospective cohort study | Inclusion: 18–65 years old men, sexually active, with proven recovery from SARS-CoV2 infection (2 negative swabs) | n = 43 | After a SARS-CoV-2 free time of approximately 35 days (range: 24–43) 25% of the men were oligo-crypto-azoospermic. Seven percent (3 patients) tested positive for at least one sample (saliva/pre-ejaculation urine, post-ejaculation urine, semen). | |
| Exclusion: inability to express informed consent, no sexual activity, ejaculatory disorders, after prostatic surgery or alpha-blockers |
Is SARS-CoV-2 sexually transmitted?
Li et al. (2020a) tried to answer this question using RT-PCR assay to detect SARS-CoV-2 in semen. Semen testing showed that 6/38 patients (15.8%) had positive results for SARS-CoV-2, including 4/15 patients (26.7%) who were in the acute stage of infection and 2/23 patients (8.7%) who were recovering. Additionally, Delaroche et al. (2021) detected positive SARS-CoV-2 PCR in semen and seminal plasma fractions within 24 hours of a positive COVID-19 test in nasopharyngeal swabs, but only in one of 32 male participants. Viral cultures were all negative.
Twelve other studies (Holtmann et al. 2020; Best et al. 2021; Burke et al. 2021; Gupta et al. 2021; Guo et al. 2021a; Ma et al. 2021; Ruan et al. 2021; Scroppo et al. 2021; Temiz et al. 2021; Dipankar et al. 2022; Donders et al. 2022; Vahidi et al. 2022) could not detect SARS-CoV-2 virus in semen samples. For example, Ma et al. (2021) used qRT-PCR to detect the SARS-CoV-2 virus in semen samples receiving negative results for all 12 male study participants. The time between semen collection and disease onset ranged from 56 days to 109 days (with a median of 78.5 days). Just like Ruan et al. (2021) (no detection of viral nucleic acid in semen samples after approximately 80 days of the last RT-PCR positive pharyngeal swab), Gupta et al. (2021) could not identify SARS-CoV-2 virus in any of the semen samples within 7 days of symptom onset or 5 days of nasopharyngeal rRT-PCR test positivity.
In the study protocol of Temiz et al. (2021), they also used the RT-PCR test for semen analysis. The results revealed that none of the patients with COVID-19 had SARS-CoV-2 in their semen samples. During that period, no standard treatment protocol had been established.
Some (Guo et al. 2021a) established strict hygienic rules to avoid virus contamination before masturbation/ejaculation. In their study, they used the RT-qPCR assay to detect SARS-CoV-2. All patients tested positive for SARS-CoV-2 RNA in the pharyngeal swabs, but tested negative in semen specimens obtained by masturbation during the COVID-19-recovery-phase. The time interval from diagnosis to semen samples acquired is approximately 32 days. Also, others (Burke et al. 2021) instructed their participants to strict hygienic rules during sampling collection. No SARS-CoV-2 was detected in the semen samples in the median of 6 days time after COVID-19 diagnosis.
The time interval of 37 days post-COVID was examined using RT-PCR (Best et al. 2021). There was no RNA detected in any participant’s semen.
Twenty men in the acute stage and 20 men in the clinical recovery stage were examined and all tested SARS-CoV-2 negative (Vahidi et al. 2022). Some (Scroppo et al. 2021) divided their study participants into two groups (mild and moderate COVID-19 disease), where SARS-CoV-2 had not been detected in any semen samples, while others (Holtmann et al. 2020) did not detect SARS-CoV-2 RNA in semen samples from either recovered (n = 18) or acute infected (n = 2) subjects in the investigated time after the end of symptoms of 32.7 days on average using RT-PCR. Dipankar et al. (2022) collected two semen samplings. All semen samples collected in the first and second (74 days after) sampling were negative for SARS-CoV-2, tested with RT-PCR.
Donders et al. (2022) performed their study during the first and second wave of COVID-19 infection in Europe, where none of the men were vaccinated against COVID-19. SARS-CoV-2 RNA was detected in none of the 120 collected semen samples with the validated SpermCOVID PCR test (RT-PCR) at a mean of 52.7 ± 35.1 days post-COVID.
There is evidence that SARS-CoV-2 is detectable in seminal fluid during the acute phase of illness. A clear effect, however, was only found in two studies (Li et al. 2020a; Delaroche et al. 2021). Whereas Gacci et al. (2021) tested three patients (7%) positive in at least one sample (saliva, pre-ejaculation urine, semen and post-ejaculation urine), 40 patients (93%) tested negative for SARS-CoV-2 RNA in a median SARS-CoV-2-free time of 35 days. Of these three positive tested men none of their partners tested positive for SARS-CoV-2 in pharyngeal, vaginal or rectal swabs, although one of these three patients tested positive in semen and had unprotected vaginal, oral and anal sex with his stable partner. All the other studies (conducted after therapy and on average after 1 month after diagnosis) could not detect SARS-CoV-2 RNA in seminal fluid so it can be assumed that SARS-CoV-2 is no longer transmitted by sperm after 1 month at the latest.
To summarise this section, it can be said that the fact that SARS-CoV-2 is barely detectable in semen makes sexual transmission (other body secretions excluded) very unlikely, especially in the case of sperm donation.
Is sperm quality reduced – and if so, how long – after SARS-CoV-2 infection?
Temiz et al. (2021) evaluated the main sperm parameters: volume, pH, sperm counts, motility, percentage of normal morphology, and seminal leukocytes. The semen parameters, except semen morphology, were within normal limits. There were significantly fewer normally formed spermatozoa in the COVID-19 patients (1–1.5%) than in the control group (3%). This effect seems to be reversible, based on checking participants 4 months to 1 year post-COVID (Aksak et al. 2022). When tested COVID-19 negative, the sperm concentration was significantly higher. No statistically significant difference was detected between the groups for sperm morphology and motility. No proband in the COVID-19 negative group was azoospermic, while four men in the COVID-19 positive group were azoospermic. By 138 days post-COVID, there was no difference seen concerning sperm morphology (Ertaş et al. 2022). In addition, there was no significant difference in semen parameters between groups in terms of sperm concentration, semen volume, and advanced motility. However, the sperm count and total motility in men with COVID-19 disease were found to be significantly lower. A decreased sperm motility was also detected (Erbay et al. 2021), dividing the participants into two subgroups (mild and moderate symptoms). Motility and vitality significantly decreased in the mild symptomatic group, while the decrease in all semen parameters including semen volume was statistically significant in the moderate symptomatic group. It was observed that fever did not contribute to this effect. This could be confirmed with a semen analysis 3 months after COVID recovery, in which they found no significant association between sperm parameters and both the previous presence of fever or COVID-19 severity (Paoli et al. 2023).
The median of semen parameters from COVID-19-recovered men was within WHO 2010 fifth percentile (Cooper et al. 2010) with no significant difference compared to the normozoospermic controls and significantly better than infertile controls. The prevalence of oligozoospermia doubles in severe cases (12.7% vs 24%) but was not statistically significant. Also, others (Guo et al. 2021a) checked for total sperm count (TSC), as well as total motile sperm count (TMSC) and sperm morphology of the patients, finding their results to be within normal ranges. The median interval from diagnosis to providing semen samples was 32 days. A contrasting effect showing that SARS-CoV-2 can affect TSC and sperm concentration was detected after a similar period (approximately 37 days post-COVID) (Best et al. 2021). The sperm concentration and TSC of men were lower when tested positive. A follow-up was done approximately 90 days later in five men who completed the analysis. They had a similar TSC compared to the initial analysis. Some (Hu et al. 2022) performed a first analysis of sperm quality after a recovery time of 83 days as well as a second follow-up at 175 days. Neither significant difference in semen parameters between male recovered patients and control subjects nor significant difference in semen parameters between the first and the second follow-up was found. The TSC showed a significant decline after a recovery time of 90 days and an improving trend after a recovery time of approximately 150 days. The total sperm motility improved after a recovery time of 120 days. The sperm quality of COVID-19-recovered patients improved after a recovery time of nearly half a year. Others (Hamarat et al. 2022) checked for TSC before (7.74 ± 3.03 month) and post-COVID (2.35 ± 1.35 month). After the COVID-19 infection there was a significant decrease in total sperm count, the mean sperm concentration, and the mean percentage of samples with normal morphology. Guo et al. (2021b) assessed the semen samples at a median time of 76 days after the appearance of symptoms and 56 days after hospital discharge. Twenty-two of the 41 patients were also tested 84 days after hospital discharge. The median time between the first and second sampling was 29 days. The sperm concentration, total sperm count, and the percentage of progressively motile and motile spermatozoa in the patients were significantly lower at first sampling, while sperm vitality and morphology were not affected. At the second sampling, the sperm concentration, TSC, and number of motile spermatozoa per ejaculate were significantly increased while the percentage of morphologically abnormal sperm was reduced.
The fact that there is no statistical difference concerning the seminal parameters in those patients with mild or moderate symptoms could be shown (Scroppo et al. 2021). Semen analysis was altered in 87% (13/15) of patients. Progressive motility was reduced in 73% of patients. Hypospermia was found in 27% of patients. There was increased viscosity in 80% of patients, with normal leukocyte counts in all collected samples. Holtmann et al. (2020) showed that patients with a moderate infection had a statistically significant impairment of sperm quality compared with men recovered from a mild infection and the control group. The individuals were divided into fever positive versus fever negative, regardless of their classification into mild and moderate and the semen was analysed. Although there were statistically significant differences regarding the complete motility, the number of immotile spermatozoa, and the volume and seminal values were all still in the normal range. Others (Pazir et al. 2021) divided the cohort into two subgroups as those with and without symptoms of fever. In the overall cohort, TMSC and total motility decreased significantly post-COVID, compared to the pre-infection values. Within the group with fever, no statistically significant difference was found between the pre- and post-infection semen parameters. In the group without fever, total motility significantly decreased post-COVID. Not only the studies mentioned above examined the effect of clinical types of COVID-19 on semen parameters, but also Ruan et al. (2021). Median interval between the last positive pharyngeal swab RT-PCR test and semen sample collection was approximately 80 days. Based on reference values, the semen characteristics of recovered COVID-19 men were within the lower reference limits. Total motility, sperm concentration, and TSC significantly declined compared with healthy controls. Different clinical types of COVID-19 have no significant difference in semen parameters, except for sperm concentration (descending trend). Men with a longer recovery time (>90 days) had a significantly lower TSC. This finding differs from the results of Gupta et al. (2021), where changes in motility and sperm count could not be found even during the active COVID-19 phase (within 7 days of symptom onset or 5 days of nasopharyngeal rRT-PCR test positivity in asymptomatic men). At the time of diagnosis of COVID-19, semen parameters showed a significant decrease in percentage of total motility, percentage of progressive motility, semen volume, and sperm morphology (Koç and Keseroğlu 2021). There was no significant difference in motility, concentration, or sperm count according to Vahidi et al. (2022), who compared men in the acute stage to men in the clinical recovery. However, a significant difference in the morphology and viability parameters could be observed (lower in men with acute disease).
Some (Li et al. 2020b) analysed semen from COVID-19 patients and showed that 39.1% (n = 9) had oligozoospermia, and 60.9% (n = 14) showed a significant increase in leukocytes in semen. Decreased sperm concentration and higher seminal levels of IL-6, TNF-a, and MCP-1, when compared to the control group, were observed. Leukocytes and cytokines could affect spermatogenesis and interfere with fertility. Also, others (Hajizadeh Maleki and Tartibian 2021) checked for markers of inflammation and oxidative stress. The semen parameters were evaluated at 10-day intervals for a maximum follow-up time of 60 days. The COVID-19 group revealed significantly higher levels of seminal plasma ACE2 enzymatic activity, TGF-β, TNF-α, IL-1β, IL-6, IL-8, IL-10, caspase-8, caspase-9, and caspase-3 activity, IFN-α, IFN-γ and reactive oxygen species, as well as lower levels of superoxide dismutase activity than those in the control group (P < 0.05). These perturbations tended to persist over time and were correlated with significant impairments in semen volume, sperm morphology, progressive motility, sperm concentration, and the number of spermatozoa. A similar period was examined by Dipankar et al. (2022), where 74 days after the first sampling, a second sampling was done. In the first sampling, semen volume, total motility, vitality, TSC, sperm concentration, percentage normal morphology, percentage cytoplasmic droplet, and fructose were significantly lower. In contrast, semen agglutination, DNA fragmentation index (DFI), liquefaction time, percentage head defect, semen viscosity, and leukocytes were increased. At the second sampling, these findings were reversed but not to the optimum level. All these findings were statistically significant (P < 0.05 for all). Thus, SARS-CoV-2 negatively affects semen parameters, including sperm DFI. In particular, the impact on the DFI was very high. DFI among all participants was more than 30% in the first sampling, with 27/30 participants showing DFI more than 30% during second sampling. The DFI was also examined and checked for sperm motility (low in 33.3%), morphology (defined as normal morphology <4%, poor sperm morphology in 16%), and DFI (assessed by sperm chromatin dispersion (SCD) test) (Ma et al. 2021). The higher the fragmentation value, the more DNA is damaged. In 4/12 patients with poor semen quality, the sperm DNA fraction percentage was increased (DFI 16.2%−23.7%). Also, a post-COVID loss of libido (25%) and a complaint about the loss of morning erection (8%) was reported. Sixteen percent had normal semen quality. Paoli et al. (2023) checked for DFI using the TUNEL assay. Three months after COVID-19 recovery, 80 patients were recruited and their mean percentage of DFI (14.1 ± 7.0%) was compared to the DFI of a normozoospermic control group published by Carlini et al. (2017) (12.8 ± 5.3%). These values were comparable. Additionally, there was no significant difference between subjects with or without fever or between COVID-19 severity groups. They only found a significant age-related correlation. Ruan et al. (2021) could not find differences checking DFI in individuals with recovery period <90 days versus >90 days after COVID-19 disease either, but the DFI in these post-COVID-19 patients in general was increased (mean DFI 18.41%).
The study with the longest period after COVID-19 disease recovery was done by Shcherbitskaia et al. (2022). The researchers compared the DFI of 17 male samples 5 months post-COVID with 22 age-matched controls using TUNEL assay. They found a TUNEL > 15 in 47.06% of men post-COVID versus 40.91% of men without a SARS-CoV-2 infection in the past. In 52.94% of men after COVID-19 they found a TUNEL < 15, which shows that COVID-19 is not always associated with increased DFI. It was shown that increased DFI and diminished semen quality in men can be caused by an imbalance in semen pro- and antioxidant components after COVID-19.
Four subgroups were defined by Al-Alami et al. (2022), who recorded seminal fluid analysis (SFA) from 354 participants (first category): only vaccinated, infected and vaccinated, neither infected nor vaccinated, and only infected. In the second category, SFA from 49 subjects before and after their infection and/or vaccination was measured. There were no statistically significant differences in the SFA records in the first data category and the second. In addition, there were no statistically significant differences between the infected patients and the uninfected patients in terms of TSC, concentration, progressive motility, liquefaction, volume, normal forms existing within the semen, and viscosity. There was no significant difference between the four groups in terms of viscosity and liquefaction, concentration, TSC, volume, and progressive motility, whereas there was a significant difference in terms of normal forms existing within the semen.
A study used 118 samples for semen analysis (Donders et al. 2022). Sperm morphology was more affected than sperm motility after COVID-19 infection. Sperm concentration was the least affected. In this study, the reduced sperm quality lasted until 52.7 ± 35.1 days post-COVID. They also tested for COVID-19 antibody titers in serum. Sperm concentration and motility decreased with increasing serum antibody titers, while DNA damage increased. In addition, the global oligoasthenicteratozoospermia severity score was strongly correlated with higher antibody levels.
To sum up, the effect of SARS-CoV-2 on sperm quality seems to be reversible after approximately 3 months.
Does COVID-19 disease have any effects on the outcome of ART?
The effect of COVID-19 on the outcome of ART was examined in Jordan (Albeitawi et al. 2022) and in Wuhan, China (Wang et al. 2022). Previous COVID-19 infection did not affect IVF/ICSI, according to the Jordanian researchers, who observed clinical pregnancy rate, implantation rate, fertilisation rate, number of oocytes retrieved, number of mature oocytes, and number and quality of embryos at day 3. The Chinese study showed no significant difference in semen quality and a similar chance of pregnancy in terms of IVF outcomes. The motility and concentration of sperm did not significantly differ. However, it seemed that infected men had fewer sperm with normal morphology, while volume, semen concentration, total number of sperm per ejaculate, progressive motility, total number of progressive motility, complete motility, total number of complete motility, immotile, total number of immotile sperms did not differ. A decreased blastocyst formation rate and available blastocyst rate were observed in the exposed group. However, no significant difference was exhibited regarding the implantation rate, clinical pregnancy rate, biochemical pregnancy rate, early miscarriage rate, mature oocyte rate, cleavage rate, normal fertilisation rate, and high-quality embryo rate.
Unfortunately, by the time of writing no study had been made about the effect of COVID-19 disease on the outcome of intrauterine insemination (IUI).
Discussion
Possibly, the presence of SARS-CoV-2 RNA in semen is explainable by different time intervals between COVID-19 infection and sample collection. It remains unclear which levels are infectious.
There was a slightly higher concentration of bacterial DNA observed in the COVID-19-positive specimen (Delaroche et al. 2021), which may indicate contamination of the sample by oropharyngeal secretions during collection. We suggest to advise for strict hygiene protocols during semen collection before assisted reproductive attempts.
We further suggest that counsellors communicate an estimated COVID-19 recovery time of 3 months (Donders et al. 2022; Paoli et al. 2023) to infertile couples who are planning parenthood or ART procedures, but the exact time interval is not yet clearly defined and so more research should be done.
Unfortunately, studies on IUI after COVID-19 disease are currently lacking, which is why only indirect speculation via sperm parameters is possible. Presumably, after sufficient recovery time (normalisation of sperm parameters), the results would becomparable to pregnancy outcomes before infection. This would have to be tested based on studies.
Conclusion
COVID-19 seems not to be a sexually transmitted disease, but there is evidence that SARS-CoV-2 is detectable in seminal fluid during the acute phase of illness. However, it can be assumed that SARS-CoV-2 is no longer transmitted in semen after 1 month at the latest.
COVID-19 infection has been shown to cause the following changes in sperm quality: altered morphology and motility, decreased sperm concentration, lower TSC per ejaculate (oligozoospermia), and a significant increase in leukocytes and cytokines in semen. These effects seem to be reversible. Couples with a desire for pregnancy should wait for the estimated recovery time of 3 months because until then their sperm quality seems to be suboptimal.
Only one study found a similar DFI in semen samples post-COVID-19 compared to controls; all the other studies showed increased DFI in patients after SARS-CoV-2 infection. Even after 5 months, individuals who had experienced COVID-19 had a higher DFI than controls, which should prompt further research concerning the health of the offspring, which could possibly be affected if the DFI is increased. This seems to be one of the most important findings of this review, opening an important field for research in the future.
Except for a decreased blastocyst formation rate and a decreased available blastocyst rate in the exposed group, COVID-19 disease does not seem to impair IVF/ICSI treatment and the outcome of ART.
Studies concerning IUI are still lacking; therefore, we advise further research on the outcome of IUI after COVID-19 infection. Also, additional research about the level of SARS-CoV-2 in semen fluid being infectious and semen quality changing over time could be helpful in clinical counselling.
Data availability
Data sharing is not applicable as no new data were generated or analysed during this study.
Author contributions
Drafting of the manuscript: JS, SK, VH. Creating of the figure: JS. Idea for the article: JS, performance of the literature search and data analysis: JS, VH. Critically revision of the work: SK. All authors have read, reviewed and approved the manuscript.
References
Aksak T, Satar DA, Bağci R, et al. (2022) Investigation of the effect of COVID-19 on sperm count, motility, and morphology. Journal of Medical Virology 94(11), 5201-5205.
| Crossref | Google Scholar |
Al-Alami ZM, Albeitawi S, ALNatsheh MS, et al. (2022) COVID-19 and semen fluid parameters, a retrospective study from infertility clinics. Life 12(12), 2076.
| Crossref | Google Scholar | PubMed |
Albeitawi S, Al-Alami ZM, Hamadneh J, et al. (2022) COVID-19 infection and vaccine have no impact on in-vitro fertilization (IVF) outcome. Scientific Reports 12(1), 21702.
| Crossref | Google Scholar |
Ata B, Vermeulen N, Mocanu E, et al. (2023) SARS-CoV-2, fertility and assisted reproduction. Human Reproduction Update 29(2), 177-196.
| Crossref | Google Scholar | PubMed |
Best JC, Kuchakulla M, Khodamoradi K, et al. (2021) Evaluation of SARS-CoV-2 in human semen and effect on total sperm number: a prospective observational study. The World Journal of Men’s Health 39(3), 489-495.
| Crossref | Google Scholar | PubMed |
Burke CA, Skytte AB, Kasiri S, et al. (2021) A cohort study of men infected with COVID-19 for presence of SARS-CoV-2 virus in their semen. Journal of Assisted Reproduction and Genetics 38(4), 785-789.
| Crossref | Google Scholar | PubMed |
Carlini T, Paoli D, Pelloni M, et al. (2017) Sperm DNA fragmentation in Italian couples with recurrent pregnancy loss. Reproductive Biomedicine Online 34(1), 58-65.
| Crossref | Google Scholar | PubMed |
Chauhan S (2020) Comprehensive review of coronavirus disease 2019 (COVID-19). Biomedical Journal 43(4), 334-340.
| Crossref | Google Scholar | PubMed |
Cooper TG, Noonan E, von Eckardstein S, Auger J, Baker HW, Behre HM, Haugen TB, Kruger T, Wang C, Mbizvo MT, Vogelsong KM (2010) World Health Organization reference values for human semen characteristics. Human Reproduction Update 16(3), 231-245.
| Crossref | Google Scholar | PubMed |
Delaroche L, Bertine M, Oger P, et al. (2021) Evaluation of SARS-CoV-2 in semen, seminal plasma, and spermatozoa pellet of COVID-19 patients in the acute stage of infection. PLoS ONE 16(12), e0260187.
| Crossref | Google Scholar |
Dipankar SP, Kumar T, Itagi ABH, et al. (2022) Semen quality in males suffering from COVID-19: a pilot study. Cureus 14(11), e31776.
| Crossref | Google Scholar | PubMed |
Donders GGG, Bosmans E, Reumers J, et al. (2022) Sperm quality and absence of SARS-CoV-2 RNA in semen after COVID-19 infection: a prospective, observational study and validation of the SpermCOVID test. Fertility and Sterility 117(2), 287-296.
| Crossref | Google Scholar | PubMed |
Erbay G, Sanli A, Turel H, et al. (2021) Short-term effects of COVID-19 on semen parameters: a multicenter study of 69 cases. Andrology 9(4), 1060-1065.
| Crossref | Google Scholar | PubMed |
Ertaş K, Eryilmaz R, Yokuş A, et al. (2022) Examining changes on testicular structure and sperm analysis of COVID-19 patients. Andrologia 54(10), e14609.
| Crossref | Google Scholar | PubMed |
Gacci M, Coppi M, Baldi E, et al. (2021) Semen impairment and occurrence of SARS-CoV-2 virus in semen after recovery from COVID-19. Human Reproduction 36(6), 1520-1529.
| Crossref | Google Scholar | PubMed |
Guo L, Zhao S, Li W, et al. (2021a) Absence of SARS-CoV-2 in semen of a COVID-19 patient cohort. Andrology 9(1), 42-47.
| Crossref | Google Scholar | PubMed |
Guo T-H, Sang MY, Bai S, et al. (2021b) Semen parameters in men recovered from COVID-19. Asian Journal of Andrology 23(5), 479-483.
| Crossref | Google Scholar | PubMed |
Gupta P, Choudhary A, Gopal G, et al. (2021) Detection of SARS-CoV2 virus using the real-time reverse transcriptase polymerase chain reaction in semen and seminal plasma from men with active COVID-19 infection – a pilot study. Indian Journal of Urology 37(4), 331-334.
| Crossref | Google Scholar | PubMed |
Hajizadeh Maleki B, Tartibian B (2021) COVID-19 and male reproductive function: a prospective, longitudinal cohort study. Reproduction 161(3), 319-331.
| Crossref | Google Scholar | PubMed |
Hamarat MB, Ozkent MS, Yilmaz B, et al. (2022) Effect of SARS-CoV-2 infection on semen parameters. Canadian Urological Association Journal 16(3), E173-E177.
| Crossref | Google Scholar | PubMed |
Holtmann N, Edimiris P, Andree M, et al. (2020) Assessment of SARS-CoV-2 in human semen – a cohort study. Fertility and Sterility 114(2), 233-238.
| Crossref | Google Scholar | PubMed |
Hu B, Liu K, Ruan Y, et al. (2022) Evaluation of mid- and long-term impact of COVID-19 on male fertility through evaluating semen parameters. Translational Andrology and Urology 11(2), 159-167.
| Crossref | Google Scholar | PubMed |
Kakodkar P, Kaka N, Baig MN (2020) A comprehensive literature review on the clinical presentation, and management of the pandemic coronavirus disease 2019 (COVID-19). Cureus 12(4), e7560.
| Crossref | Google Scholar | PubMed |
Koç E, Keseroğlu BB (2021) Does COVID-19 worsen the semen parameters? Early results of a tertiary healthcare center. Urologia Internationalis 105(9–10), 743-748.
| Crossref | Google Scholar |
Li D, Jin M, Bao P, et al. (2020a) Clinical characteristics and results of semen tests among men with coronavirus disease 2019. JAMA Network Open 3(5), e208292.
| Crossref | Google Scholar | PubMed |
Li H, Xiao X, Zhang J, et al. (2020b) Impaired spermatogenesis in COVID-19 patients. EClinicalMedicine 28, 100604.
| Crossref | Google Scholar | PubMed |
Ma L, Xie W, Li D, et al. (2021) Evaluation of sex-related hormones and semen characteristics in reproductive-aged male COVID-19 patients. Journal of Medical Virology 93(1), 456-462.
| Crossref | Google Scholar | PubMed |
Moshrefi M, Ghasemi-Esmailabad S, Ali J, et al. (2021) The probable destructive mechanisms behind COVID-19 on male reproduction system and fertility. Journal of Assisted Reproduction and Genetics 38(7), 1691-1708.
| Crossref | Google Scholar | PubMed |
Paoli D, Pallotti F, Anzuini A, et al. (2023) Male reproductive health after 3 months from SARS-CoV-2 infection: a multicentric study. Journal of Endocrinological Investigation 46(1), 89-101.
| Crossref | Google Scholar | PubMed |
Pazir Y, Eroglu T, Kose A, et al. (2021) Impaired semen parameters in patients with confirmed SARS-CoV-2 infection: a prospective cohort study. Andrologia 53(9), e14157.
| Crossref | Google Scholar | PubMed |
Ruan Y, Hu B, Liu Z, et al. (2021) No detection of SARS-CoV-2 from urine, expressed prostatic secretions, and semen in 74 recovered COVID-19 male patients: a perspective and urogenital evaluation. Andrology 9(1), 99-106.
| Crossref | Google Scholar | PubMed |
Scroppo FI, Costantini E, Zucchi A, et al. (2021) COVID-19 disease in clinical setting: impact on gonadal function, transmission risk, and sperm quality in young males. Journal of Basic and Clinical Physiology and Pharmacology 33(1), 97-102.
| Crossref | Google Scholar | PubMed |
Shcherbitskaia AD, Komarova EM, Milyutina YP, et al. (2022) Oxidative stress markers and sperm DNA fragmentation in men recovered from COVID-19. International Journal of Molecular Sciences 23(17), 10060.
| Crossref | Google Scholar | PubMed |
Temiz MZ, Dincer MM, Hacibey I, et al. (2021) Investigation of SARS-CoV-2 in semen samples and the effects of COVID-19 on male sexual health by using semen analysis and serum male hormone profile: a cross-sectional, pilot study. Andrologia 53(2), e13912.
| Crossref | Google Scholar | PubMed |
Vahidi S, Nabi A, Alipoor H, et al. (2022) Effect of coronavirus disease (COVID-19) on human semen: no evidence of coronavirus in semen of patients. BioMed Research International 2022, 6204880.
| Crossref | Google Scholar | PubMed |
Wang W, Xu Y, Gao R, et al. (2020) Detection of SARS-CoV-2 in different types of clinical specimens. JAMA 323(18), 1843-1844.
| Crossref | Google Scholar |
Wang M, Hu J, Huang B, et al. (2022) Investigating the impact of SARS-CoV-2 infection on basic semen parameters and in vitro fertilization/intracytoplasmic sperm injection outcomes: a retrospective cohort study. Reproductive biology and endocrinology: RB&E 20(1), 46.
| Crossref | Google Scholar |