

Older adults’ experiences of a community wellness program (Connect 60+) that focused on physical activity and social connections: a qualitative exploratory study
Tammy Weselman A * , Chiara Naseri A B , Sharmila Vaz A , Janet Beilby C , Luke Garswood D , Hilary O’Connell E and Anne-Marie Hill A B
A * , Chiara Naseri A B , Sharmila Vaz A , Janet Beilby C , Luke Garswood D , Hilary O’Connell E and Anne-Marie Hill A B
A The University of Western Australian, School of Allied Health, Crawley, WA 6009, Australia.
B Western Australian Centre for Health and Ageing, University of Western Australia, Crawley, WA 6009, Australia.
C Curtin University, School of Allied Health, Bentley, WA 6102, Australia.
D Connect Victoria Park, Victoria Park, WA 6100, Australia.
E Independent Living Australia, Perth, WA 6000, Australia.
Abstract
Being physically active and socially connected is positively associated with healthy aging. Older adults living in the community may be at risk of social isolation and reduced physical activity, especially in recent times due to COVID-19. There are many programs that offer opportunities for evidence-based physical activity or social connection; however, there is a lack of programs that include both. The objective of this study was to explore the lived experience of older adults who participated in Connect 60+ – a program that promoted exercise and social activities – delivered from a community hub that could be attended either in person or online.
A qualitative study that used descriptive phenomenology was conducted. A purposive sample of 13 older adults (age ≥65 years) was recruited to take part in semistructured telephone interviews to discuss barriers and enablers to program engagement. Data were analysed using thematic analysis.
The overarching theme was that participating in Connect 60+ was an enjoyable and encouraging experience for participants. The program enabled them to increase their physical activity and build social connections within their community. The main themes that enabled engagement were: (1) an enabling program design, (2) developing new connections in the community, and (3) experiencing motivation to engage. A few barriers were identified, including difficulties connecting online and lack of male attendance.
Wellness programs delivered in community hubs may facilitate older adults to increase their engagement in both physical and social activity. The program appeared to impact positively on participants’ motivation, with some participants reporting that they had sustained their behaviour changes since program completion. To address identified barriers, easy to use online technology is recommended, and strategies to promote male attendance.
Keywords: community hubs, healthy aging, older adults, online, physical activity, qualitative, social connections, strength and balance.
Introduction
The World Health Organization (World Health Organization 2015) defines healthy aging as the process of maintaining the functional ability that enables wellbeing in older age. However, the nature of the COVID-19 pandemic has forced many older adults to remain at home rather than engage in healthy aging behaviours of being functionally (both physically and socially) active out in the community (Brooke and Jackson 2020; Gaertner et al. 2021). This has significant health and cost implications for older populations and for health services, because of global population growth (Reich et al. 2020). In 2020, there were approximately 4.2 million (16%) Australians aged ≥65 years, and this number is expected to grow to between 21 and 23% by 2066 (Australian Government: Australian Institute of Health and Welfare 2021).
Exercise is an established, evidence-based, healthy aging strategy (Ylitalo et al. 2020) that is recommended for prevention of chronic illness, functional decline and falls (Chodzko-Zajko et al. 2009; Palmer et al. 2018). However, <50% of older adults engage in the recommended amount of at least 150 min per week (Bull et al. 2020). Social connectedness is another healthy aging strategy that enables wellbeing, and reduces the risk of premature mortality and negative health outcomes, such as depression and anxiety (Holt-Lunstad et al. 2015; Courtin and Knapp 2017), and has been identified as central to an individual’s perception of their wellbeing (Diener and Seligman 2004; Santini et al. 2020). However, approximately 25% of older adults are reported to be socially isolated, meaning this also negatively impacts on their health and wellbeing (National Academies of Sciences, Engineering, and Medicine 2020).
Community-based healthy aging programs have the potential to fill these gaps in a holistic manner. Community hubs can offer a convenient, local space for older adults to engage in healthy aging strategies of exercise and socially connecting with others (Markle-Reid et al. 2018; Salman et al. 2021). Older adults are much more likely to continue with, and make social connections, in a physical activity program they enjoy (Creighton et al. 2022). In a synthesis of research on community hubs performed between 2000 and 2020, it was found that community hubs offer a range of services throughout the community; however, of the 18 studies reviewed, six of these were aimed at social care for older adults with chronic illness or disability, and none of them included physical activity (Manis et al. 2022). Another review suggested that physical activity was particularly good for vulnerable older people, as it improved their functional ability; however, it also noted that physical activity alone did not reduce loneliness (Shvedko et al. 2018). Therefore, both social interaction and physical activity is required. Expert consensus around the world supports use of The World Health Organization’s ‘Integrated Care for Older People’ (ICOPE) approach, which highlights the importance of health and social care interventions being delivered at all service levels, including in the local community (Briggs and de Carvalho 2018).
A recently developed program aimed to fill this gap through designing a wellness program through a partnership between researchers, older members of a community hub and health professionals. This community-based research partnership led to the design and pilot of a wellness program (Connect 60+) for community-dwelling older adults at risk of social isolation and declining levels of physical activity during the COVID-19 pandemic (Naseri et al. 2022). It was aligned with international recommendations for healthy aging (Abbasi et al. 2021). A quantitative program evaluation demonstrated that participants increased the frequency of social connections and exercise completed per week (Naseri et al. 2022). However, it was also important to seek participants’ feedback to identify their experiences of the program, including their perspectives about possible barriers and enablers to its success, to assist future implementation and program growth (Greenhalgh and Papoutsi 2019). More broadly, examining older adults’ perspectives on wellness programs can enhance understanding of how these programs could be used to promote healthy aging strategies (Talley et al. 2019).
The objective of the study was to explore the lived experiences of older community-dwelling adults who participated in Connect 60+, a wellness program that promoted engagement in exercise and social connectedness, at a community hub. We aimed to understand the impact of the program on participants’ engagement in healthy aging strategies of exercise and social connectedness, and to identify the barriers and enablers for older adults engaging in these strategies.
Methods
Study design
The study took a descriptive phenomenological approach to explore the meaning of participants’ individual experiences (Matua and Van Der Wal 2015) during the Connect 60+ program and their reflections 12 months after the program was finished. Descriptive phenomenology was chosen to faithfully describe participants’ experiences with the program, with the aim of exploring the impact of the program on participants, and understanding barriers and enablers to the program’s success.
Participants and setting
A purposive sample (n = 13) was recruited from the 47 participants who had completed the wellness program in a community hub in Perth, Western Australia (Naseri et al. 2022). Inclusion criteria for the program and for this study were: being aged ≥60 years, cognitive function that enabled participation in the program and ability to give informed consent (assessed as scoring >7/10 using the Abbreviated Mental Test Score (Hodkinson 2012)), and ability to speak and comprehend English. This was to ensure sufficient engagement with the intervention and ability to operate the online technology. There was no additional incentive offered to those who attended online, and they met the same inclusion criteria, so would have been able to attend either via Zoom or in person. Most participants who attended online did so for the novel experience. The primary researcher recruited participants in a purposeful manner, using a stratified sampling approach (Liamputtong 2013) that gave consideration to in-person and online attendance, age, and sex. Participants were telephoned and invited to take part, and a time was arranged for the interview. None of the participants declined the interview; however, some were unable to be reached by phone, even after several attempts. Theoretical saturation was confirmed through consensus with a second researcher reviewing the transcribed data and primary researcher’s notes (Carpenter 2013).
The wellness program
The planning and delivery of Connect 60+ used a community-based participatory research approach (Kwon et al. 2018) that uses local member preferences and motivations to facilitate their engagement in the program (Ward et al. 2018). A comprehensive 9-week healthy aging and wellness program, Connect 60+, was delivered from a community hub between July and September 2020. To support program attendance, participants living in the hub’s local neighbourhood did not pay a fee to attend (either in person or online). Participants chose to attend either in person or remotely via Zoom (https://zoom.us/). Participants who were enrolled online participated by joining a live stream of classes as they occurred in the community hub main hall. Online connections were facilitated by the primary researcher (TW). Attendance was once a week for 3 h. Sessions included 60 min of strength and balance exercises, according to guideline recommendations for this type of exercise in improving and maintaining health among older people (Sherrington et al. 2020; Ylitalo et al. 2020). Participants used the remaining time in each session to have morning tea and engage in weekly wellness activities, such as ballroom dancing, chair yoga or storytelling. Online participants were encouraged to join in with social activities using the online platform, by the primary researcher being present online with them, using breakout rooms for discussion and ensuring activity facilitators included online participants. On the days where the activity took place outside, such as pole walking and nature walks, all participants were able to attend. Wellness activities were designed according to community member interests and availability of local facilitators; and encompassed the domains of wellness (physical, social, intellectual, emotional, environment, vocational and spiritual; International Council on Active Ageing 2001)
Data collection procedure
Data were collected through two sources – weekly feedback gathered after each session and telephone interviews after program completion. Collecting data from multiple sources to use in the analysis was a form of method triangulation that aimed to improve the credibility of the study (Nowell et al. 2017). The weekly feedback from participants, either gathered before or after each event, was recorded in the researcher’s diary. Additionally, the researcher used the diary throughout the program to keep track of the program’s progress (Nowell et al. 2017). Member checking was undertaken throughout and at the completion of the interviews to ensure the responses were being captured adequately, with the aim of enhancing the credibility of the results (Creswell and Miller 2000; Doyle 2007).
Telephone interviews took place over 2 weeks in November 2021, 1 year after the Connect 60+ program was completed. Each interview was between 20 and 30 min in duration and was undertaken by the primary researcher (TW). An individual phone interview was selected to allow participants a convenient and confidential way to discuss their experiences openly and honestly (Schofield and Forrester-Knauss 2013). The primary researcher was involved throughout the program and had established a genuine rapport with participants.
The interviews were designed to explore three key areas: (1) participants’ experiences with the wellness program in general; (2) participants’ lived experiences of undertaking the wellness program, including any barriers and enablers to engaging with the program activities; and (3) participants’ attitudes and beliefs about engaging in physical activity and connecting with others socially.
Data analysis
Interviews were recorded and transcribed verbatim to gain an accurate understanding of participants’ responses (Braun and Clarke 2013). The primary researcher (TW) transcribed the first two interviews to evaluate whether they accurately captured participant experiences (Creswell 2014, p. 193). Minor adjustments were made to the order and wording of the questions to improve the interview flow. The remainder of the interviews were professionally transcribed. The primary researcher (TW) examined these and checked the wording against the interviews for clarity if required. Data from participants’ weekly feedback were coded with the transcriptions, and researcher comments from the researcher’s diary were also used in the analysis process.
Data were thematically analysed using an inductive approach (Braun and Clarke 2006). Each interview was read thoroughly twice to enable the researcher to become familiar with the material (Braun and Clarke 2006; Nowell et al. 2017). During this phase the researcher aimed to gain a rich understanding of the content and took notes regarding the meanings of the data, as well as initial codes to be used in the next phase. The researcher sorted the data into three broad groups (participants’ experiences with the program; barriers and enablers to partaking; attitudes and beliefs) to which the initial codes were applied. Each section was then searched for codes, key words and phrases that stood out to the researcher (Braun and Clarke 2006).
Two researchers (TW and CN) first coded data independently, then conferred to discuss the codes and reach consensus. They subsequently grouped codes to create candidate themes. These were then examined to ensure all coded data were represented by the themes and created a picture of the whole dataset. During this process, exemplar quotes were chosen to be used in this report, and those were checked against the raw data to ensure they were not taken out of context (Nowell et al. 2017). Finally, all three researchers (TW, CN, AMH) met to discuss and reach consensus on the final themes and to create the thematic map (Braun and Clarke 2006).
Ethical considerations
Ethics approval was obtained from the Human Research Ethics Committee, Curtin University, Perth, Western Australia (HRE2020-0398). All participants provided written informed consent to participate, including undertaking follow-up telephone interviews. Additional verbal consent from participants was gained at the start of each telephone interview.
Results
Semistructured phone interviews were completed with eight women and five men (age range 65–86 years). Four of the participants had joined the Connect 60+ program online, the rest attended the hub in person. Seven participants lived in the local hub neighbourhood. The demographic information of participants is presented in Table 1. A total of 13 interviews were completed, after which saturation was reached, with all the main variations of the phenomena recurring and no new themes being identified (Liamputtong 2013). A thematic map schematically demonstrating theme relationships and coding exemplars is presented in Fig. 1. Main themes that captured participants’ experiences were identified, and within these themes both positive and negative experiences were found. These assisted to understand barriers and enablers to participants’ engagement in the program.
| Characteristic | n (%) | |
|---|---|---|
| Age (years) | ||
| 60–64 | 1 (7) | |
| 65–74 | 7 (53) | |
| 75–79 | 3 (23) | |
| 80–86 | 2 (15) | |
| Sex, female | 8 (61) | |
| Highest level of education | ||
| Grade 10 | 2 (15) | |
| Grade 12 | 3 (23) | |
| Diploma | 3 (23) | |
| Degree | 5 (38) | |
| Have children | 12 (92) | |
| Living arrangements | ||
| Alone | 7 (53) | |
| With partner | 4 (30) | |
| With other family | 2 (15) | |
| Has a pet | 5 (38) | |
| Attendance | ||
| In person | 9 (69) | |
| Online | 4 (30) | |
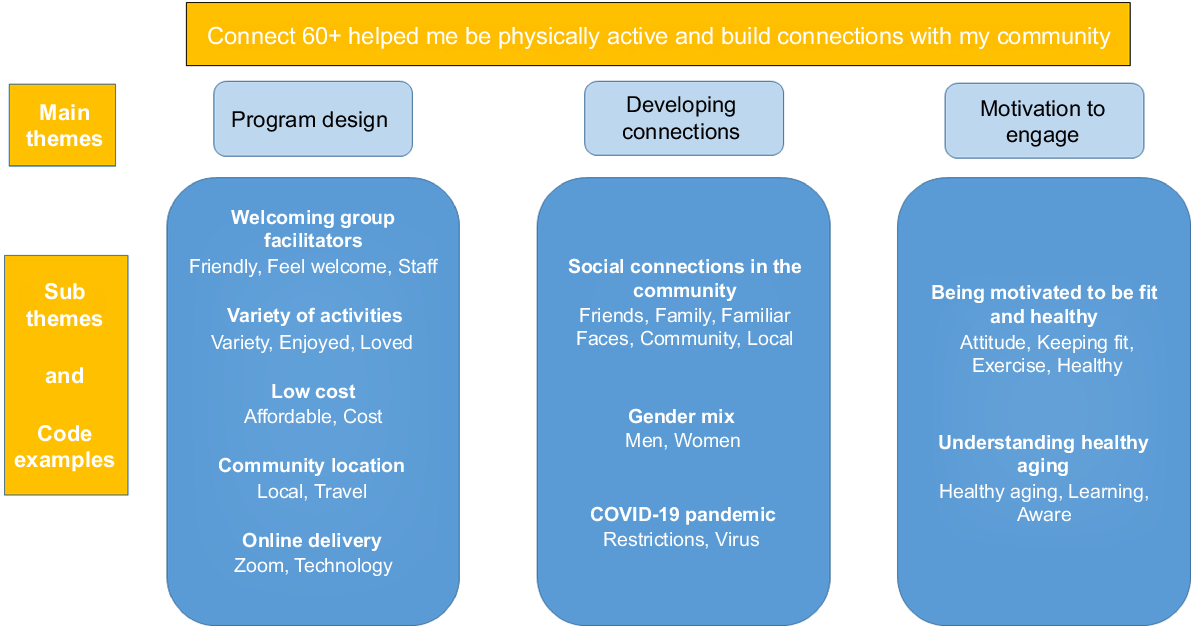
Overarching theme: Connect 60+ helped me be physically active and build connections with my community
The overarching theme identified that participants experienced Connect 60+ as enabling and encouraging them to be physically active, and to socially connect within their community. The response to the program was overwhelmingly positive, with a limited number of negative experiences or problems described. Participants experienced the hub as being a welcoming space that they enjoyed and looked forward to attending. The low cost, convenient location and variety of activities were integral to its success. Overarchingly, participants spoke about ‘my community’, and described the importance of the friendships and social connections that their attendance at the hub and participation in the program created and, in some cases, had sustained after program completion. Participants found motivation throughout their time in the program in many things: the program itself, their families, and an aspiration to be fit and healthy as they aged.
Main theme 1: Program design
Participants strongly concurred that they found the Connect 60+ program appealing. The program was welcoming, promoted enjoyment, familiarity and motivation to be a part of their local community, whether online or in person. It encouraged them to engage in new activities, and build and sustain their levels of participation in a broader range of activities.
Participants reported that the presenters made the program an enjoyable experience (this resulted in a code of ‘friendly’), and was an enabler for participation in the wellness activities with one participant stating, ‘… (name) is just a good facilitator; he is fabulous…’ (p45/F/online). Another participant commented that, ‘I feel the staff are very supportive and very friendly … they make everyone feel welcome’ (p4/F/in person). One participant contrasted her positive experiences of Connect 60+ with another group she previously attended and stressed the importance of feeling welcomed to a community group, ‘I think that the people who greet you at the front door make or break the program, they had quite a domineering lady there that made me feel quite inadequate so I never went back’ (p7/F/in person).
The Connect 60+ program offered a variety of wellness activities in addition to the exercise class and morning tea. The range of activities was mentioned by multiple participants as being a key reason for enjoying the program. Activities ranged from storytelling to singing, ‘I enjoyed the variety of things the most’ (p24/M/in person). For example, pole walking was a favourite activity for many of the participants, and was the first time that most had experienced it, ‘It’s just a case of finding what you enjoy, I particularly liked the pole walking’ (p7/F/in person). On this day the researcher recorded that, ‘The pole walking is clearly a crowd favorite, everyone loved getting outside and the mood was really positive’ (researcher diary, 4 September 2021).
The membership fees being waived for people in the local area was perceived by participants as an enabler, as it allowed older adults to participate in the program regardless of their income. One participant described ‘…a great opportunity to try different things at minimal or zero cost’ (p47/M/online). The cost benefit was contrasted by another participant, ‘I think gym costs are one of the biggest problems today’ (p30/M/in person).
The location of the hub was an advantage for participants living in the local area, ‘I think that’s a motivator, I need to have something I can do that’s close to my doorstep…’ (p7/F/in person). This benefit was highlighted by one participant, who said they really enjoyed the program, but was also a barrier for engagement for some ‘…unfortunately it was a little bit far for me to come regularly for activities’ (p14/F/in person).
There were four participants interviewed who attended the program using the online platform. Some reported this as a barrier to engagement, ‘I did it on Zoom and I could not say that this made me feel connected to the community… though it was strange as the camera was set-up to the side of the people, so they didn’t look straight [at the camera]’ (p36/F/online). Others found the online connection a more positive experience. One participant said, ‘I hadn’t used Zoom before but I can do it now, I’m glad I learned how to do this during the program’ (p41/M/online). Another shared the online benefits for others, ‘… I think it’s good for people who don’t have a big social circle or who don’t have many family members’ (p45/F/online). Another negative experience for online participants were were some technical difficulties early in the program, with the online connection, and this was rectified within the week. The researcher noted in the second week that, ‘now the technical problems are resolved, the Zoomers were able to connect, I saw them participating in the exercise and they all tried very hard and most seemed to enjoy it’ (researcher diary, 7 August 2021).
Main theme 2: Developing connections
Developing new social connections during Connect 60+ and feeling more connected to ‘my community’ was identified by participants as a positive experience and an enabler to participation in healthy aging strategies.
Connections and building friendships were dominant enabling themes. For example, participants spoke positively about making new friends at the community hub and wanting to strengthen those friendships, ‘The good thing is you get to connect with the same people in all the classes’ (p36/F/online). One participant described the social connection as their main reason for being involved in the program, ‘I joined the community hub specifically to keep myself socially engaged, because I know this is a really important part of maintaining your health and well-being’ (p47/F/online).
As well as making friends within the hub, many participants shared that the program helped them feel more connected to the community in general, ‘…whole area felt quite inclusive’ (p7/F/in person). Others expressed similar sentiments, ‘I feel more a part of the community now,’ (p18/M/in person) another saying, ‘I think that whole community activities were very good and drew a lot of more people into it’ (p30/M/in person).
Most of the participants of Connect 60+ were female. One female participant commented that she was inspired by the older women attending the program, stating that ‘there are a lot of women, that’s always good, a couple of the women were quite mature, and that’s inspiring’ (p8/F/in person). Men, in contrast, identified the lack of other men as a possible barrier to engagement, with a male participant reporting that ‘it tends to be more women, it would be better to have more men attend, so they could benefit from what the program offers’ (p24/M/in person).
The program was conducted during the COVID-19 pandemic and this affected participation due to social distancing mandates in public areas, which altered some older adults’ experiences of the program. One participant commented that they would have preferred to be there in person for a better experience, as only a limited number of participants were allowed in the hub at one time. ‘There were noticeable restrictions … during the program’ (p41/M/online). However, program organisers did their best to ensure that there was as little impact as possible, the researcher noted, ‘Some members were disappointed they couldn’t come in person because of the COVID space restrictions, but everyone mostly understood and felt okay with it’ (Researcher Diary, 14 August 2020). One participant had a more positive outlook, explaining that she worked harder to maintain connections during lockdown, she stated, ‘I think during COVID-19 lockdown, I forged stronger connections with the people’ (p8/F/in person).
Theme 3: Motivation to engage
There was a dominant theme of participants feeling motivated by Connect 60+ to continue to participate in healthy aging activities related to exercise and socially connecting. Furthermore, some participants reported that they perceived they were more open to engaging in novel activities or changing their behaviour in the 12 months since completing the program.
Being motivated to stay fit and healthy was frequently named as an enabler for participation. Some participants were motivated by their family history; for example, ‘…my family has a history of heart problems, so I want to keep as active as I can’ (p4/F/in person). Other participants spoke of changing their priorities with daily activities to address their general wellbeing, and staying healthy and active. One participant highlighted her shift in priorities by stating ‘I just get out and exercise, without worrying about cleaning the dusty house’ (p4/F/in person), and another said, ‘I am trying to change that old mind-set of being so negative and re-phrase it to a positive, so not be so hard on myself, and remind myself anything is better than no exercise’ (p14/F/in person).
Participants reported that during the program and in the 12 months following, they continued to be involved in healthy aging activities., ‘I was already a member before the program, but I increased my membership to Gold, so I could attend more activities during the week’ (p8/F/in person). Others were inspired to seek out new activities, ‘it gave me the inspiration to go and look for what I wanted in other groups and clubs that I could join’ (p7/F/in person).
The intensity of the physical activity at Connect 60+ was mentioned by some participants as a barrier to engagement, with one participant sharing, ‘I wasn’t terribly good with exercises because of rheumatoid arthritis’ (p41/M/online). However, others, who were more capable, preferred to attend other physical activities that challenged their ability. This was exemplified by a participant who stated that ‘it wasn’t quite active enough for me’ (p2/F/in person).
The education provided by Connect 60+ enabled participants to increase their health knowledge, and feel more motivated to participate in healthy aging activities during and since the program. One participant reported that the program, ‘… gave education and tips on how to live better… making me more aware of how important it was to keep doing these activities, even when you don’t feel like it’ (p18/M/in person). Another stated, ‘I learned that it’s okay to do a bit more exercise than I normally would have done’ (p17/F/in person).
Many participants enjoyed learning about different aspects of wellness. However, not all the activities provoked positive responses. Activities that required members to break into groups for discussion on topics that required personal reflections and memories, such as storytelling, stimulated some negative feedback about this experience, ‘I’m not into where you have to discuss your feelings… it’s not for me’ (p4/F/in person). Some participants mentioned to the researcher that timing of the activities within the program was not ideal. The researcher noted that, ‘some people mentioned to me that the getting to know you type of activities done today should have been done earlier in the program’ (researcher diary, 11 September 2021).
Discussion
This study found that older adults reported their experiences of the wellness program as being very positive and, in some cases, it facilitated sustained change in their motivation to engage in physical activity and make social connections, and even seek out new activities. Healthy aging strategies, such as exercise, are importan,t because increasing one’s level of physical activity can help prevent chronic disease, functional decline and falls (Palmer et al. 2018; Naseri et al. 2020). As <50% of older adults engage in recommended amounts of physical activity, increasing participation is an important means of improving healthy aging in the older population (Piercy et al. 2018; Bull et al. 2020).
Participants were also motivated to increase social connections, which is important to address social isolation and loneliness as risk factors for reduced function (York Cornwell and Waite 2009; Shankar et al. 2017; Robins et al. 2018). Although social isolation and loneliness are connected, they are not the same thing. Social isolation refers to an objective lack of social interaction and networks, and loneliness describes the subjective feeling of not having one’s social needs met (Berg-Weger and Morley 2020; Van As et al. 2022). The Connect 60+ program offered participants an environment to create relationships, which in turn helped them develop the confidence to build relationships outside the program. Other research has found older adults prioritise social connections as a wellness strategy (Reich et al. 2020; Santini et al. 2020). Older people have also previously reported that they value social activities as a way to be connected to the community in a friendly atmosphere that is based on trust and security (Salman et al. 2021).
Participants who attended in person reported that a key enabling feature of Connect 60+ was its accessibility. The low cost, friendly staff and convenient location, near a main street with cafes, shops and buses, were factors of success. The participants spoke positively about the group facilitators at the hub. The low cost was especially important, as older adults tend to have a lower or fixed income compared with other sections of the community (Ylitalo et al. 2020), making some exercise programs inaccessible. Previous studies have also found that affordable and accessible community hubs enable older adults to get involved in their local community (Palmer et al. 2018; Ylitalo et al. 2020).
Participants commented that the program encouraged and motivated them by providing physical activity that they found enjoyable (Dacey et al. 2008). However, there was one participant who found the exercise too vigorous for them, which was a barrier to engagement. Older adults have reported previously that barriers to engaging in exercise include feeling that exercise is too difficult, health problems that impact on participation and low self-efficacy (Hill et al. 2011). Most participants also became motivated to learn about healthy aging, which increases self-efficacy to engage in healthy aging strategies (Notthoff et al. 2017). By addressing the domains of wellness, Connect 60+ included multiple determinants of health known to sustain healthy aging and independence (Strout et al. 2016, 2018; Tuason et al. 2021).
During the past few years of the COVID-19 pandemic, social isolation, loneliness, reduced levels of physical activity and difficulties in maintaining care have been identified as major health risks for older adults (Gaertner et al. 2021). However, even during mandated lockdowns, it is important to maintain a normal routine for one’s physical health and general wellbeing (Strout et al. 2016; Bentlage et al. 2020). One way to stay connected during these times is via technology (Chen and Schulz 2016). Although only a small number of participants joined online, this study showed that technology can assist people to engage with and join activities from a community hub. However, some participants reported difficulty with the online experience, which highlighted the importance of maximising accessibility for a positive user experience and supporting older adults in using technology during online wellness activities (Chen and Schulz 2016; Silvius et al. 2020). A report showed that in 2018, approximately 40% of older adults had not used the internet in the 3 months prior. Reasons for this included not feeling confident with the technology (Australian Bureau of Statistics 2020).
Strengths and limitations
A strength of the present study was the methods of triangulation used to increase the trustworthiness of the study (Nowell et al. 2017). Data were collected from a range of sources and analysed by three researchers. The primary researcher was also involved in the running of the weekly program, keeping an audit trail that increased the dependability of findings (Creswell and Miller 2000; Nowell et al. 2017). Member checking ensured that participants’ experiences were truly captured (Creswell 2014, p. 201), and in the final stages of manuscript drafting, a simplified copy of the results section was sent to three participants to confirm that it was a fair and accurate representation of their experiences of the program. A limitation of the study was that telephone interviews were completed 12 months after the study, due to limitations caused by COVID-19 pandemic restrictions impacting on research timelines. This may have affected participants’ recall of their experiences either in a positive or negative manner. However, participants were enthusiastic to describe the impact of the program on their experiences in the 12 months following its completion, as well as their original experiences when undertaking the program. This added richness to the understanding of how their experience during the program had impacted on their lives.
A genuine rapport was built during the program between the primary researcher and the participants, which was important to enable participants to feel safe to share their views (Braun and Clarke 2013). However, this may also have been a limitation, as participants may have felt reluctant to provide negative responses (Ramcharan 2013). There were only a small number of online participants compared with those who did the program in person, which limits the finding to this study and may not be generalisable to older community-dwelling people. However, purposive sampling was used to gain insight across the sample and maximise our understanding of the data in this study (Braun and Clarke 2013).
Conclusion
Connect 60+ was successful in supporting participants to engage in healthy aging strategies for being physically active and socially connected. The study contributes valuable evidence towards developing innovative programs that support older adults to continue to enjoy good health and remain socially connected as they age in their community (Manz et al. 2018; Salman et al. 2021). Although participants concurred strongly that the program was a positive experience and had a positive impact on their lives, there were some barriers to engagement. Strategies to address barriers include encouraging more men to join, optimising online technology for a better user experience, ensuring exercises are suited to all fitness levels, and continuing to provide a broad range of wellness and social activities to suit more preferences. This study demonstrated that wellness programs delivered from a community hub can enable physical activity and social connections due to the accessibility, variety of activities, and providing a welcoming environment in the local community.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Declaration of funding
The authors have not received funding for this study. Professor Anne-Marie Hill receives career support through a National Health and Medical Research Council of Australia Investigator EL2 Grant.
Author contributions
CN, AMH and TW conceptualised the study design and research protocol with ongoing expertise and support from JB, SV, HO and LG. AMH, CN and TW led trial management. TW and CN led data collection and management, and site procedure, in consultation with LG. TW and CN led statistical analyses. TW led the drafting of all sections of the manuscript in consultation with CN, AMH and SV. All authors critically revised the manuscript for important intellectual content, and read and approved the final version of the manuscript.
References
Abbasi M, Khera S, Dabravolskaj J, Chevalier B, Parker K (2021) The seniors’ community hub: an integrated model of care for the identification and management of frailty in primary care. Geriatrics 6, 18.
| Crossref | Google Scholar |
Australian Bureau of Statistics (2020) ‘Use of information technology by people with disability, older people and primary carers.’ (Australian Bureau of Statistics: Canberra, ACT, Australia) Available at https://www.abs.gov.au/articles/use-information-technology-people-disability-older-people-and-primary-carers [Verified 8 July 2022]
Australian Government: Australian Institute of Health and Welfare (2021) Older Australians. Australian Institute of Health and Welfare, Canberra, ACT, Australia. Available at https://www.aihw.gov.au/reports/older-people/older-australia-at-a-glance/contents/summary [Verified 8 July 2022]
Bentlage E, Ammar A, How D, Ahmed M, Trabelsi K, Chtourou H, Brach M (2020) Practical recommendations for maintaining active lifestyle during the COVID-19 pandemic: a systematic literature review. International Journal of Environmental Research and Public Health 17, 6265.
| Crossref | Google Scholar |
Berg-Weger M, Morley JE (2020) Loneliness and social isolation in older adults during the COVID-19 pandemic: implications for gerontological social work. The Journal of Nutrition Health & Aging 24, 456-458.
| Crossref | Google Scholar |
Braun V, Clarke V (2006) Using thematic analysis in psychology. Qualitative Research in Psychology 3, 77-101.
| Crossref | Google Scholar |
Briggs AM, de Carvalho IA (2018) Actions required to implement integrated care for older people in the community using the World Health Organization’s ICOPE approach: a global Delphi consensus study. PLoS ONE 13, e0205533.
| Crossref | Google Scholar |
Brooke J, Jackson D (2020) Older people and COVID-19: isolation, risk and ageism. Journal of Clinical Nursing 29, 2044-2046.
| Crossref | Google Scholar |
Bull FC, Al-Ansari SS, Biddle S, Borodulin K, Buman MP, Cardon G, Carty C, Chaput J-P, Chastin S, Chou R, Dempsey PC, DiPietro L, Ekelund U, Firth J, Friedenreich CM, Garcia L, Gichu M, Jago R, Katzmarzyk PT, Lambert E, Leitzmann M, Milton K, Ortega FB, Ranasinghe C, Stamatakis E, Tiedemann A, Troiano RP, van der Ploeg HP, Wari V, Willumsen JF (2020) World Health Organization 2020 guidelines on physical activity and sedentary behaviour. British Journal of Sports Medicine 54, 1451-1462.
| Crossref | Google Scholar |
Chen Y-RR, Schulz PJ (2016) The effect of information communication technology interventions on reducing social isolation in the elderly: a systematic review. Journal of Medical Internet Research 18, e18.
| Crossref | Google Scholar |
Chodzko-Zajko WJ, Proctor DN, Fiatarone Singh MA, Minson CT, Nigg CR, Salem GJ, Skinner JS (2009) Exercise and physical activity for older adults. Medicine & Science in Sports & Exercise 41, 1510-1530.
| Crossref | Google Scholar |
Courtin E, Knapp M (2017) Social isolation, loneliness and health in old age: a scoping review. Health and Social Care in the Community 25, 799-812.
| Crossref | Google Scholar |
Creighton RM, Paradis KF, Blackburn NE, Tully MA (2022) Group-based physical activity interventions targeting enjoyment in older adults: a systematic review. Journal of Ageing and Longevity 2, 113-129.
| Crossref | Google Scholar |
Creswell JW, Miller DL (2000) Determining validity in qualitative inquiry. Theory into Practice 39, 124-130.
| Crossref | Google Scholar |
Dacey M, Baltzell A, Zaichkowsky L (2008) Older adults’ intrinsic and extrinsic motivation toward physical activity. American Journal of Health Behavior 32, 570-582.
| Crossref | Google Scholar |
Diener E, Seligman MEP (2004) Beyond money: toward an economy of well-being. Psychological Science in the Public Interest 5, 1-31.
| Crossref | Google Scholar |
Doyle S (2007) Member checking with older women: a framework for negotiating meaning. Health Care for Women International 28, 888-908.
| Crossref | Google Scholar |
Gaertner B, Fuchs J, Möhler R, Meyer G, Scheidt-Nave C (2021) Older people at the beginning of the COVID-19 pandemic: a scoping review. Journal of Health Monitoring 6, 2-37.
| Crossref | Google Scholar |
Greenhalgh T, Papoutsi C (2019) Spreading and scaling up innovation and improvement. BMJ 365, l2068.
| Crossref | Google Scholar |
Hill A-M, Hoffman T, McPhail S, Beer C, Hill KD, Brauer SG, Haines TP (2011) Factors associated with older patients’ engagement in exercise after hospital discharge. Archives of Physical Medicine and Rehabilitation 92, 1395-1403.
| Crossref | Google Scholar |
Hodkinson HM (2012) Evaluation of a mental test score for assessment of mental impairment in the elderly. Age and Ageing 41, iii35-iii40.
| Crossref | Google Scholar |
Holt-Lunstad J, Smith TB, Baker M, Harris T, Stephenson D (2015) Loneliness and social isolation as risk factors for mortality: a meta-analytic review. Perspectives on Psychological Science 10, 227-237.
| Crossref | Google Scholar |
International Council on Active Ageing (2001) ‘Seven dimensions of wellness.’ (International Council on Active Ageing: Vancouver, BC, Canada) Available at https://www.icaa.cc/activeagingandwellness/wellness.htm [Verified 8 July 2022]
Kwon SC, Tandon SD, Islam N, Riley L, Trinh-Shevrin C (2018) Applying a community-based participatory research framework to patient and family engagement in the development of patient-centered outcomes research and practice. Translational Behavioral Medicine 8, 683-691.
| Crossref | Google Scholar |
Manis DR, Bielska IA, Cimek K, Costa AP (2022) Community-informed, integrated, and coordinated care through a community-level model: a narrative synthesis on community hubs. Healthcare Management Forum 35, 105-111.
| Crossref | Google Scholar |
Manz K, Mensink GBM, Jordan S, Schienkiewitz A, Krug S, Finger JD (2018) Predictors of physical activity among older adults in Germany: a nationwide cohort study. BMJ Open 8, e021940.
| Crossref | Google Scholar |
Markle-Reid M, Ploeg J, Fraser KD, Fisher KA, Bartholomew A, Griffith LE, Miklavcic J, Gafni A, Thabane L, Upshur R (2018) Community program improves quality of life and self-management in older adults with diabetes mellitus and comorbidity. Journal of the American Geriatrics Society 66, 263-273.
| Crossref | Google Scholar |
Matua GA, Van Der Wal DM (2015) Differentiating between descriptive and interpretive phenomenological research approaches. Nurse Researcher 22, 22-27.
| Crossref | Google Scholar |
Naseri C, McPhail SM, Haines TP, Morris ME, Shorr R, Etherton-Beer C, Netto J, Flicker L, Bulsara M, Lee D-CA, Francis-Coad J, Waldron N, Boudville A, Hill A-M (2020) Perspectives of older adults regarding barriers and enablers to engaging in fall prevention activities after hospital discharge. Health and Social Care in the Community 28, 1710-1722.
| Crossref | Google Scholar |
Naseri C, Beilby J, Vaz S, Xu D, Garswood L, O’Connell H, Hill A-M (2022) Connect 60+ a wellness program for older adults delivered online from a community hub. Progress in Community Health Partnerships [in press].
| Google Scholar |
Notthoff N, Reisch P, Gerstorf D (2017) Individual characteristics and physical activity in older adults: a systematic review. Gerontology 63, 443-459.
| Crossref | Google Scholar |
Nowell LS, Norris JM, White DE, Moules NJ (2017) Thematic analysis: striving to meet the trustworthiness criteria. International Journal of Qualitative Methods 16, 1609406917733847.
| Crossref | Google Scholar |
Palmer K, Marengoni A, Forjaz MJ, Jureviciene E, Laatikainen T, Mammarella F, Muth C, Navickas R, Prados-Torres A, Rijken M, Rothe U, Souchet L, Valderas J, Vontetsianos T, Zaletel J, Onder G (2018) Multimorbidity care model: recommendations from the consensus meeting of the Joint Action on Chronic Diseases and Promoting Healthy Ageing across the Life Cycle (JA-CHRODIS). Health Policy 122, 4-11.
| Crossref | Google Scholar |
Piercy KL, Troiano RP, Ballard RM, Carlson SA, Fulton JE, Galuska DA, George SM, Olson RD (2018) The physical activity guidelines for Americans. Journal of the American Medical Association 320, 2020-2028.
| Crossref | Google Scholar |
Reich AJ, Claunch KD, Verdeja MA, Dungan MT, Anderson S, Clayton CK, Goates MC, Thacker EL (2020) What does “Successful Ageing” mean to you? – systematic review and cross-cultural comparison of lay perspectives of older adults in 13 countries, 2010–2020. Journal of Cross-Cultural Gerontology 35, 455-478.
| Crossref | Google Scholar |
Robins LM, Hill KD, Finch CF, Clemson L, Haines T (2018) The association between physical activity and social isolation in community-dwelling older adults. Aging & Mental Health 22, 175-182.
| Crossref | Google Scholar |
Salman K, Turek JM, Donovan C (2021) Community health and wellness fair: a strategy for assessment of social determinants of health, inclusion and engagement of newcomers. Journal of Community Health 46, 527-537.
| Crossref | Google Scholar |
Santini ZI, Jose PE, York Cornwell E, Koyanagi A, Nielsen L, Hinrichsen C, Meilstrup C, Madsen KR, Koushede V (2020) Social disconnectedness, perceived isolation, and symptoms of depression and anxiety among older Americans (NSHAP): a longitudinal mediation analysis. The Lancet Public health 5, e62-e70.
| Crossref | Google Scholar |
Shankar A, McMunn A, Demakakos P, Hamer M, Steptoe A (2017) Social isolation and loneliness: prospective associations with functional status in older adults. Health Psychology 36, 179-187.
| Crossref | Google Scholar |
Sherrington C, Fairhall N, Wallbank G, Tiedemann A, Michaleff ZA, Howard K, Clemson L, Hopewell S, Lamb S (2020) Exercise for preventing falls in older people living in the community: an abridged Cochrane systematic review. British Journal of Sports Medicine 54, 885-891.
| Crossref | Google Scholar |
Shvedko A, Whittaker AC, Thompson JL, Greig CA (2018) Physical activity interventions for treatment of social isolation, loneliness or low social support in older adults: a systematic review and meta-analysis of randomised controlled trials. Psychology Sport and Exercise 34, 128-137.
| Crossref | Google Scholar |
Silvius HAM, Tak ECPM, Mook-Kanamori DO, Vos HMM, Numans ME, Chavannes NH (2020) Effects of technology use of ageing in place: the iZi pilots. International Journal of Environmental Research and Public Health 17, 5052.
| Crossref | Google Scholar |
Strout KA, David DJ, Dyer EJ, Gray RC, Robnett RH, Howard EP (2016) Behavioral interventions in six dimensions of wellness that protect the cognitive health of community-dwelling older adults: a systematic review. Journal of the American Geriatrics Society 64, 944-958.
| Crossref | Google Scholar |
Strout K, Ahmed F, Sporer K, Howard EP, Sassatelli E, Mcfadden K (2018) What are older adults wellness priorities? A qualitative analysis of priorities within multiple domains of wellness. Healthy Aging Research 7, e21.
| Crossref | Google Scholar |
Talley KMC, Cheung C, Mathiason MA, Schorr E, McMahon S, Wyman JF (2019) Aging adults’ preferences for wellness program activities and delivery characteristics: a cross-sectional survey. Topics in Geriatric Rehabilitation 35, 289-299.
| Crossref | Google Scholar |
Tuason MT, Güss CD, Boyd L (2021) Thriving during COVID-19: predictors of psychological well-being and ways of coping. PLoS ONE 16, e0248591.
| Crossref | Google Scholar |
Van As BAL, Imbimbo E, Franceschi A, Menesini E, Nocentini A (2022) The longitudinal association between loneliness and depressive symptoms in the elderly: a systematic review. International Psychogeriatrics 34, 657-669.
| Crossref | Google Scholar |
Ward M, Schulz AJ, Israel BA, Rice K, Martenies SE, Markarian E (2018) A conceptual framework for evaluating health equity promotion within community-based participatory research partnerships. Evaluation and Program Planning 70, 25-34.
| Crossref | Google Scholar |
World Health Organization (2015) World report on ageing and health. World Health Organization, Geneva, Switzerland. Available at https://apps.who.int/iris/handle/10665/186463 [Verified 8 July 2022]
Ylitalo KR, Cox W, Gutierrez M, Benavidez G, Umstattd Meyer MR, Niceler B, Griggs JO (2020) A prescription for wellness: exercise referrals at a federally qualified health center. Journal of Primary Care & Community Health 11, 1-9.
| Crossref | Google Scholar |
York Cornwell E, Waite LJ (2009) Social disconnectedness, perceived isolation, and health among older adults. Journal of Health and Social Behavior 50, 31-48.
| Crossref | Google Scholar |