

Year in review: communicable disease surveillance, NSW, 2008
Communicable Diseases Branch, NSW Department of Health
NSW Public Health Bulletin 20(10) 141-151 https://doi.org/10.1071/NB09021
Published: 9 November 2009
Abstract
In this issue, we present our annual review of notifiable diseases reported in New South Wales (NSW) residents. For greater depth of detail, refer to Tables 2–6, which show disease-specific data reported by: year of onset; month of onset; area health service (AHS); and age group and sex.
|

|

|

|

|

|
Trends
Among the 53 573 notifications of medical conditions by doctors, hospital staff and laboratory staff in NSW residents in 2008, highlights included:
Conditions most frequently reported
-
Chlamydia: 14 043 cases (201 per 100 000 population), with the highest crude rates by geographical area in the Greater Western (Broken Hill region), South Eastern Sydney Illawarra (Randwick region), Sydney South West (Camperdown region) and Hunter New England (Tamworth region) AHSs.
-
Pertussis: 8756 cases (126 per 100 000 population), with the highest crude rates in the North Coast (Lismore region), Sydney West (Penrith and Parramatta regions), South Eastern Sydney Illawarra (Wollongong region) and Greater Western (Dubbo region) AHSs.
-
Hepatitis C: 3916 cases (56 per 100 000 population), with the highest crude rates in the Greater Western (Broken Hill and Dubbo regions), North Coast (Lismore region) and Sydney South West (Camperdown region) AHSs.
-
Hepatitis B: 2638 cases (38 per 100 000 population) with the highest crude rates in the Sydney South West (Camperdown and Liverpool regions) and Sydney West (Parramatta region) AHSs.
-
Salmonella infection: 2263 cases (32 per 100 000 population) with the highest crude rates in the North Coast (Lismore region) and Northern Sydney Central Coast (Gosford and Hornsby regions) AHSs.
Conditions with the most meaningful declines in the number of notifications compared with previous years
-
Hepatitis A: cases have more than halved in number since 2002 (69 cases in 2008 compared with 149 in 2002 and 421 in 1999). This may be due in part to the introduction of a commercial vaccine in the 1990s. Travel to countries where Hepatitis A is endemic was the most commonly reported risk factor for disease acquisition in 2008.
-
Hepatitis C: cases have decreased by over 50% in number in the last 10 years (3916 cases in 2008 compared with 8598 cases in 1999). The cause of this decline is unclear. It may reflect a real decrease in transmission related to prevention programs, or it may reflect a decrease in hepatitis C testing.
-
Meningococcal serogroup C disease: notifications continue to decline (nine cases reported for 2008), largely due to the introduction of meningococcal C vaccination in late 2003.
-
Meningococcal serogroup B disease: notifications have decreased steadily over the past few years. In 2008, there were 49 cases reported, compared with 103 in 2002. The reason for this decrease is unclear.
-
Rubella: notifications have decreased from 191 cases in 2000 to 17 cases in 2008. This may be due to higher rates of immunisation over the past decade.
Conditions with the most meaningful increases in the number of notifications compared with previous years
-
Pertussis has shown the greatest increase in the number of infections, up from 2100 in 2007 to 8756 in 2008; this reflects a large, statewide outbreak that continues in 2009, as well as improved diagnostic technology.
-
Chlamydia has been reported at the highest rate since it became a notifiable disease in 1998 (14 043 cases in 2008), reflecting a long-standing trend of increases in notifications of this disease.
-
The number of Ross River virus notifications increased from 844 in 2007 to 1155 in 2008. This is consistent with past cyclical fluctuations in Ross River virus activity.
-
The number of Salmonella infections showed a small decline compared with the previous year (2263 in 2008 compared with 2555 in 2007), but numbers remain high compared with the 10-year average.
-
The number of verotoxigenic Escherichia coli infections remained higher than usual, with 17 cases reported in 2008, compared with an average of four cases per year for the 10-year period prior to 2007. All cases were investigated and no epidemiological links were identified.
-
The number of cases of infectious syphilis remained at comparatively high levels in 2008, reflecting an outbreak among men who have sex with men residing in inner-Sydney.
Conditions least frequently reported
There were no reported cases of anthrax, avian influenza, botulism, chancroid, diphtheria, lyssavirus, plague, polio, severe acute respiratory syndrome (SARS), smallpox, typhus, viral haemorrhagic fever or yellow fever in NSW in 2008. One case of tetanus was reported.
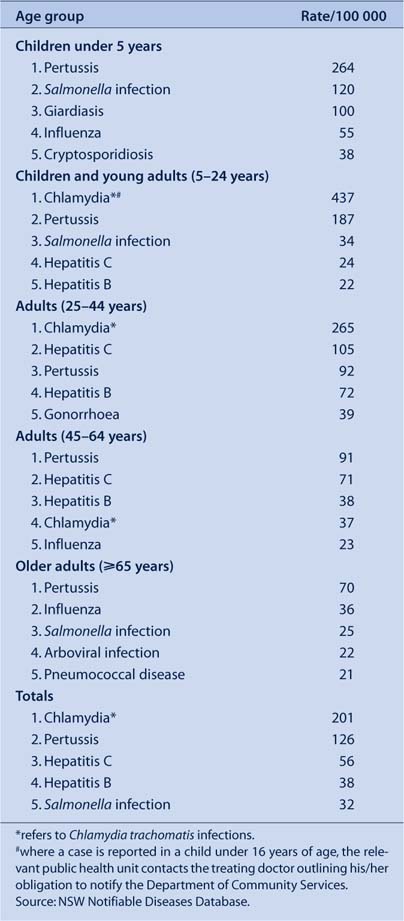
Top five notifiable diseases
Rates for the most commonly reported notifiable diseases for each age group and geographical area of residence at the time of notification are presented in Figure 1 and Table 1. These lists indicate the relative importance of notifiable diseases only and should not be used to indicate the spread of all infectious diseases in NSW. It should also be noted that these rates are heavily influenced by testing practices and, in many instances, do not necessarily indicate the true or relative incidence in the community. Finally, these lists do not include institutional gastrointestinal outbreaks because comprehensive demographic data are not collected for such outbreaks.

|
Geographical distribution of notifiable diseases
-
Chlamydia trachomatis infection was the most commonly reported infection across NSW, with the highest rates observed in rural areas, followed by regional and metropolitan areas.
-
The rate of pertussis infections was highest in rural areas, particularly in northern NSW, followed by metropolitan and regional areas.
-
Rates of hepatitis C infection were comparable across rural, regional and metropolitan areas. Most of these cases represent chronic infection rather than acute hepatitis C acquisition and as such may not accurately reflect the recent spread of hepatitis C in the community.
-
Arboviral infections were more commonly reported in people residing in rural and regional areas than in metropolitan areas.
-
Tuberculosis was most frequently reported in metropolitan areas, and was rare in rural regions.
-
Higher rates of bloodborne diseases and sexually transmissible infections (e.g. chlamydia, syphilis and hepatitis B and C) were reported for Justice Health compared with the rest of NSW. This is likely to be related to testing for these diseases on entry into correctional facilities. Within the prison population, hepatitis C was the most commonly reported infection, likely related to risk factors among people who are incarcerated.
Age distribution of notifiable diseases
-
Gastrointestinal and respiratory diseases were most commonly reported in children aged under 5 years. This may be partly due to high testing rates for these diseases in children.
-
Pertussis notifications were highest in the group aged 5–24 years, affected both sexes equally, and were also high in females aged 25–44 years, perhaps reflecting increased testing and/or infection of women of child-bearing age.
-
Pertussis was also the most commonly reported notifiable disease in adults aged 65 years and older.
-
Chlamydia was most common in the group aged 5–24 years, with females accounting for twice as many notifications as males. This is likely to be partly due to higher screening rates for chlamydia in women.
Outbreaks and threats
Several notable disease outbreaks and threats were reported in 2008 in NSW. These included:
-
An outbreak of pertussis which first appeared in northern NSW. The highest age-specific incidence was seen in children aged under 1 year.3
-
There were five strains of influenza circulating in 2008, with an epidemic of influenza B. An earlier peak of influenza than seen in previous years may have been due to the influx of overseas travellers for World Youth Day in July.
-
There were a number of discrete foodborne salmonella outbreaks, several of which were traced back to raw egg products in a range of foods.3
-
There were several clusters of measles cases from January 2008, with 38 cases reported between January and June, compared with four cases reported in the same period in 2007.1,2 One was associated with an English language school, one was associated with an under-immunised population in the Blue Mountains, and one was associated with transmission in an emergency department.
Conclusions
Controlling the spread of communicable diseases remains a priority for NSW. Vaccine-preventable diseases and sexually transmissible infections are of particular concern. This is exemplified by the re-emergence of infectious syphilis amongst men who have sex with men and the high rates of chlamydia in young adults.
The transmission of vaccine-preventable diseases, including measles and pertussis, also increased in NSW in 2008 compared with previous years. This highlights the challenge of increasing vaccination rates among adolescents and young adults, as well as the importance of promoting and maintaining high vaccination rates in infants.
We thank all those general and specialist medical practices, laboratories, hospitals, schools, child-care centres, and others who have notified diseases of public health significance to their local public health units for investigation and control.
[1] NSW Department of Health. Communicable Diseases Report, NSW, for January and February 2008. N S W Public Health Bull 2008; 19(3–4): 78–83.
| Crossref | GoogleScholarGoogle Scholar | PubMed |

[2] NSW Department of Health. Communicable Diseases Report, NSW, for July and August 2008. N S W Public Health Bull 2008; 19(9–10): 186–90.
| Crossref | GoogleScholarGoogle Scholar |
[3] NSW Department of Health. Communicable Diseases Report, NSW, for November and December 2008. N S W Public Health Bull 2009; 20(1–2): 31–5.
| Crossref | GoogleScholarGoogle Scholar | PubMed |